Abstract
Background: In 2024, the United States experienced a record-breaking 48,150 transplants, a 23.3% annual increase since 2020. Post-transplant complications are a significant challenge to long-term graft survival and quality of life for patients. Supplementation with omega-3 fatty acids (n-3) may provide benefits for solid-organ transplant (SOT) recipients by improving lipid profiles and reducing blood pressure. However, there is no consensus on the most effective regimen.
Objective: The purpose of this study was to assess the optimal use of n-3 supplementation in adult SOT recipients, with the goal of improving clinical guidelines.
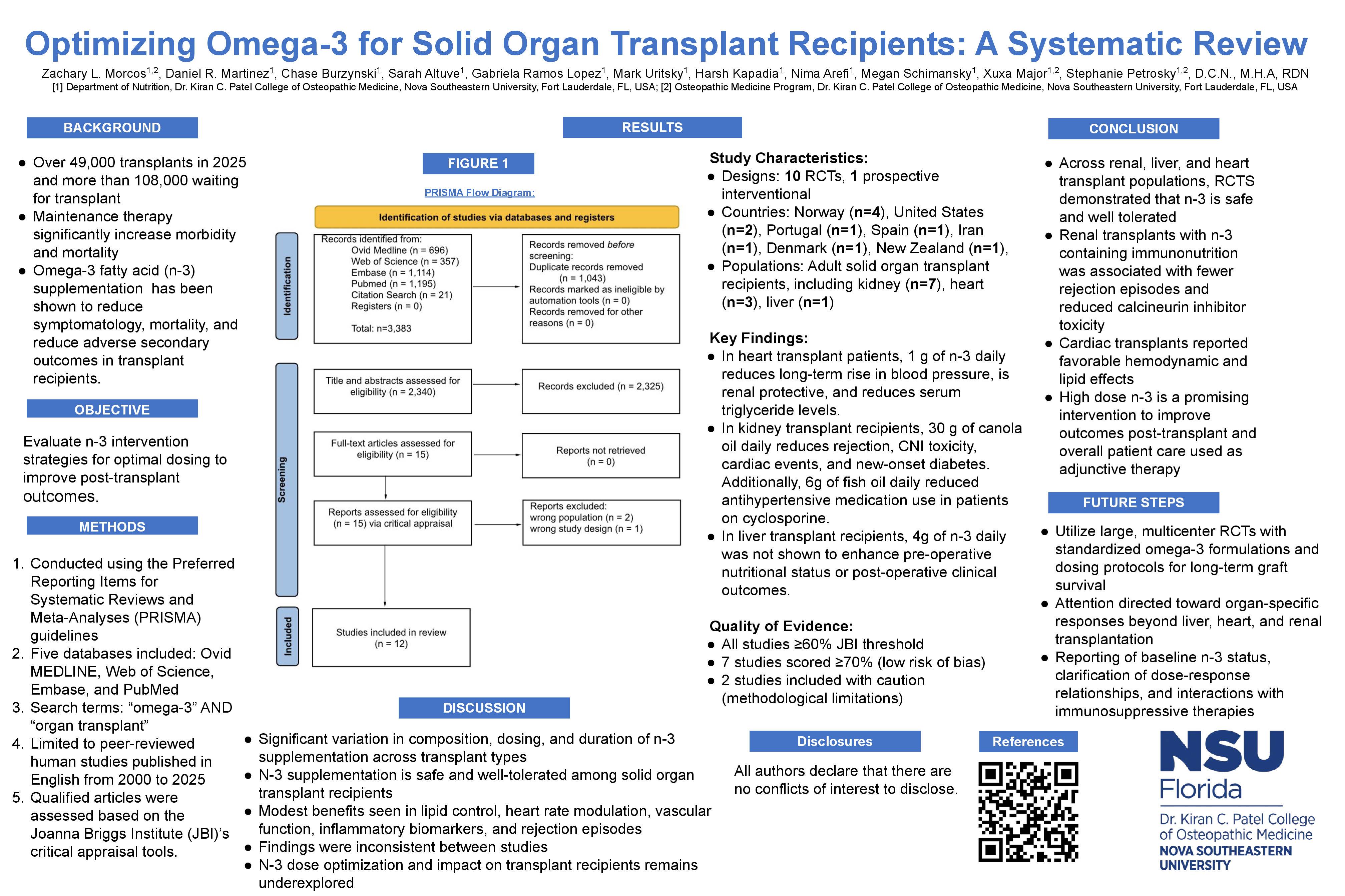
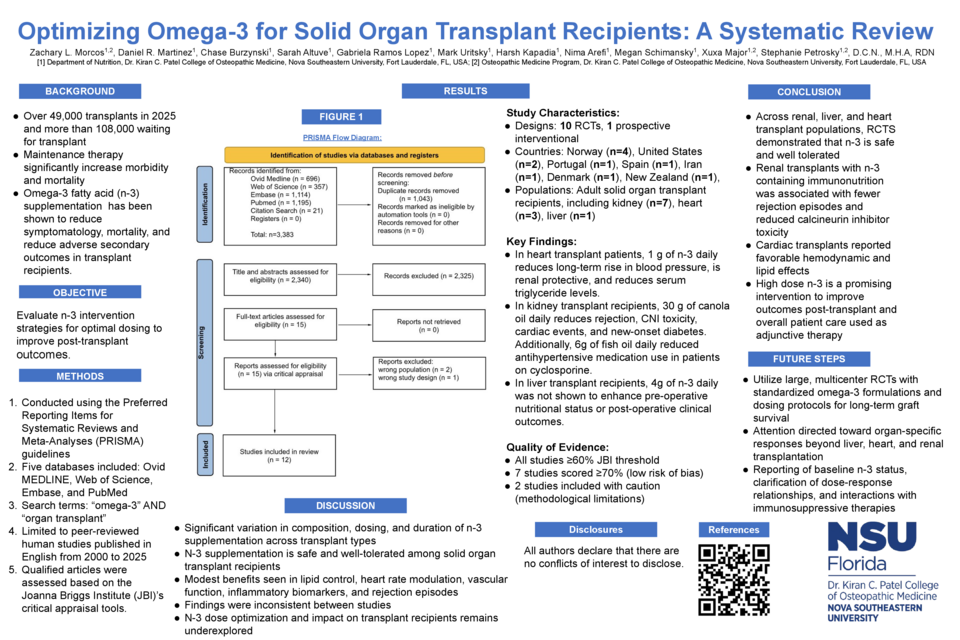
Methods: A systematic review was conducted according to PRISMA guidelines. Databases searched include Ovid MEDLINE, Web of Science, Embase, and PubMed. Search terms included “omega-3” AND “organ transplant.” The search was limited to peer-reviewed human studies published in English from 2000 to 2025. All original research evaluated the use of n-3 on postoperative outcomes in solid-organ transplant recipients.
Results: 12 studies met inclusion. Majority of n-3 supplementation began postoperatively, only one study administered perioperatively. Doses ranged from 1 to 6 grams of n-3 daily for up to three years post procedures. In heart transplant (n=3), 1g of n-3 mixtures containing EPA, DHA and antioxidants, resulted in significant decrease in triglyceride levels and stabilization of blood pressure. In liver transplantation (n=1), perioperative immunonutrition did not improve preoperative nutritional status or postoperative complication rates. In kidney transplantation, most trials (n=5) demonstrated no significant benefit of n-3 supplementation on quality of life, renal function, acute rejection, lipid profile, oxidative stress, or bone mineral density. One study on kidney transplant, reported 6g of fish oil daily with vitamins E and A, to significantly reduce the use of antihypertensive medication and improved lipid profiles. Two studies on kidney recipients, administering n-3 in the form of canola oil, reported significant reduction in organ rejection, calcineurin toxicity, new onset diabetes mellitus, and cardiac events.
Conclusion: This review highlights a significant variation in composition, dosing, and duration of n-3 supplementation across transplant types, limiting direct assessment of therapeutic benefit. However, evidence suggests that high dose n-3 is a promising intervention to improve outcomes post-transplant and overall patient care when used as adjunctive therapy. Future research should further elucidate the effects of dosing and formulations, thereby supporting the development of standardized clinical guidelines.