Abstract
BACKGROUND
Hemophagocytic lymphohistiocytosis (HLH) is a rare and life-threatening syndrome of hyperinflammation caused by an uncontrolled immune activation. Primary HLH is most commonly a pediatric disease with genetic etiologies and secondary HLH usually arises in adults with a history of infection or malignancy. Because the primary form of HLH is more prevalent and easily identifiable because of its genetic nature, secondary HLH has often been overlooked. The general pathophysiology of secondary HLH is also still not entirely understood and is not commonly diagnosed, due to the fact that its clinical manifestations overlap with those of an infection or sepsis. We present the case of a 68-year-old woman who presented with hypotension, diarrhea, and worsening fatigue. Lab studies revealed abnormalities consistent with HLH diagnostic criteria. The patient was treated with the HLH-94 regimen, consisting of etoposide and dexamethasone.
CASE PRESENTATION
A 68-year-old female presented to the clinic, accompanied by her daughter, with the complaint of chills. Over the past 5 days, she developed diarrhea and became weaker and lightheaded. She had a history of hypertension and hyperlipidemia. Vitals demonstrated sinus tachycardia. The extremities were warm without edema. There was no evidence of hepatomegaly or splenomegaly. The CBC at the time of admission demonstrated a WBC count of 10.56, indicating neutrophilia and monocytosis. Normocytic normochromic anemia and moderate thrombocytopenia were also noted. A CMP reported hyponatremia, hypokalemia, a BUN of 26, and creatinine of 2.21. There was also hypoalbuminemia and a slight increase in lipase. AST was 103 and ALT was 45 with a slight elevation of alkaline phosphatase. The patient’s ferritin was 9408, folate was 8.3, and B12 was >2000. The triglycerides were 277, lactic acid was 1.3, and TSH was normal. There were no significant culture isolates or positive PCR panels.
DISCUSSION
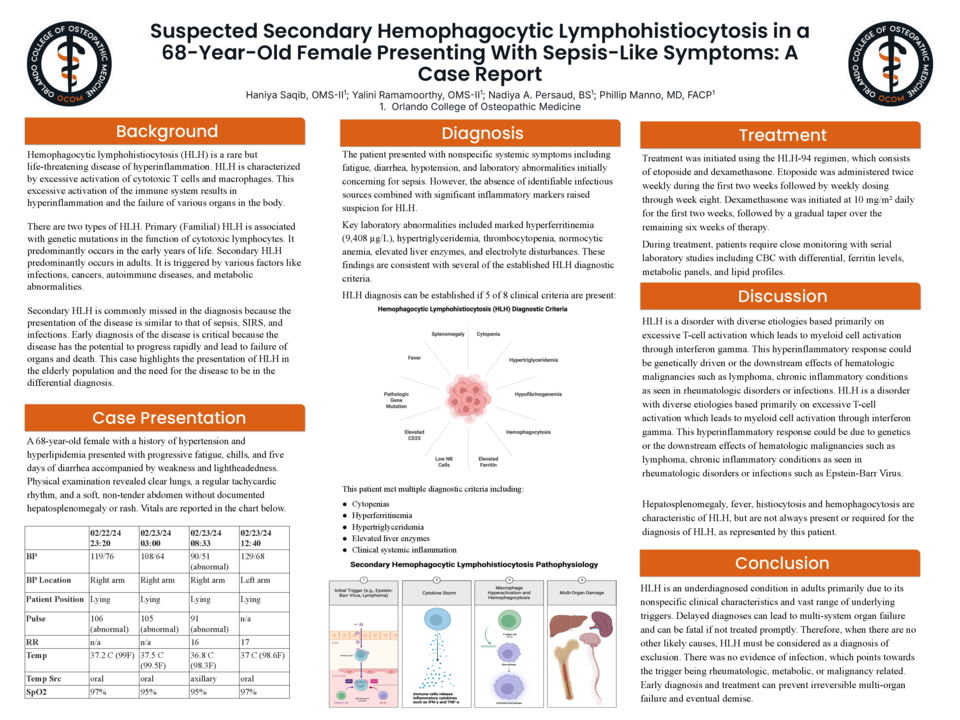
HLH is a disorder with diverse etiologies based primarily on excessive T-cell activation which leads to myeloid cell activation through interferon gamma. This hyperinflammatory response could be genetically driven or the downstream effects of hematologic malignancies such as lymphoma, chronic inflammatory conditions as seen in rheumatologic disorders or infections such as Epstein-Barr Virus. Although there are a constellation of findings, this patient has the findings of thrombocytopenia, hyperferritinemia (9408 ug/L), hypertriglyceridemia (277 mg/dL), elevated liver enzymes (AST 103) and other laboratory findings. As often is the case, ascertaining the underlying trigger is very important, especially in the setting of malignancy where the approach to treatment would be different. Hepatosplenomegaly, fever, histiocytosis, and hemophagocytosis are characteristic of HLH, but are not always present or required for the diagnosis of HLH, as represented by this patient.




