Abstract
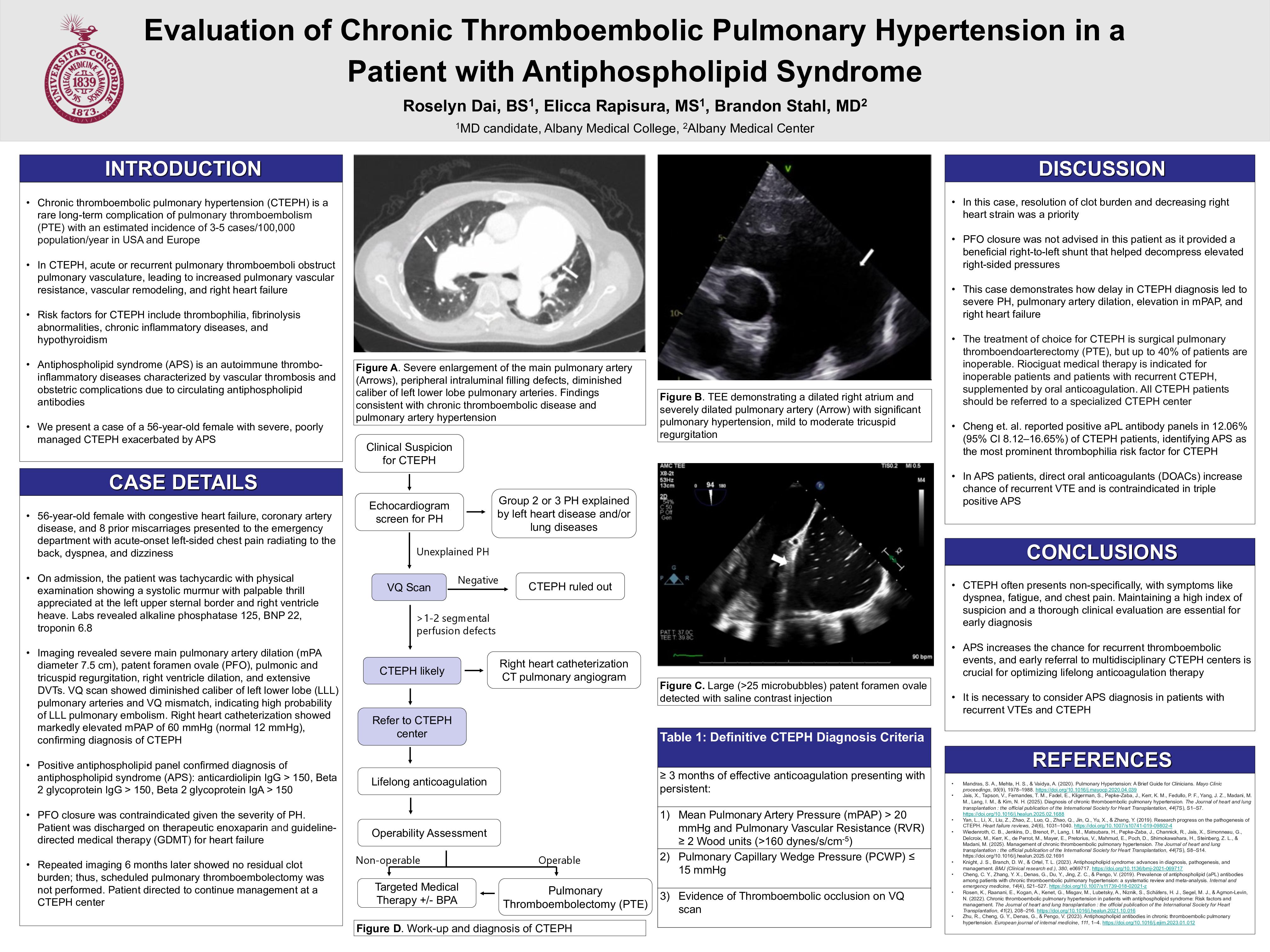
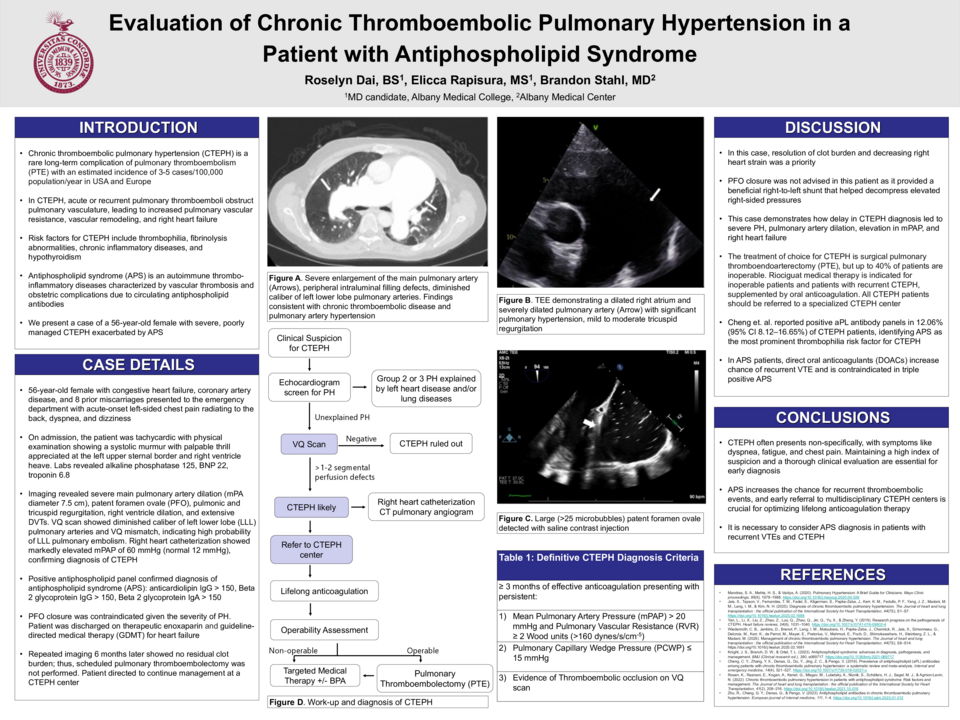
Case: A 56-year-old female with a history of coronary artery disease and congestive heart failure presented to the emergency department with acute-onset left-sided chest pain radiating to the back, dyspnea, and dizziness. On examination, she was tachycardic with a systolic murmur and palpable thrill appreciated at the left upper sternal border. Imaging revealed a severely dilated main pulmonary artery, high-probability VQ mismatch in the left lower lobe. Echocardiogram showed evidence of severe pulmonary hypertension, tricuspid and pulmonary regurgitation, and a patent foramen ovale. PFO closure was contraindicated given the severity of her pulmonary hypertension. Right heart catheterization showed markedly elevated mean pulmonary artery pressure of 60 mmHg (normal 12 mmHg). Duplex ultrasonography demonstrated extensive deep vein thrombosis. The patient also had a history of eight prior miscarriages, which raised suspicion for an underlying hypercoagulable disorder. Subsequent antiphospholipid antibody (aPL) testing was positive, confirming the diagnosis of antiphospholipid syndrome (APLS). Therapeutic enoxaparin and guideline-directed medical therapy for heart failure were initiated. She was seen at a CTEPH center six months later, and repeat imaging showed no residual clot burden.
Discussion: This case illustrates the relationship between hypercoagulability and chronic thromboembolic disease. APLS is a known risk factor for recurrent pulmonary embolism and thus development of CTEPH. Around 12% of CTEPH patients test positive for aPL, therefore recognizing APLS early is critical for initiating lifelong therapeutic anticoagulation. Additionally, this case shows the complexity of managing CTEPH. Our patient did not meet criteria for PTE as repeat imaging showed no persistent thrombi suitable for surgical removal. Moreover, closure of the PFO was not advised as it provided a beneficial right-to-left shunt that helped decompress elevated right-sided pressures. This case highlights the importance of timely diagnosis and an individualized treatment plan in patients with CTEPH and underlying APLS to enhance patient outcomes and prevent disease progression.