Abstract
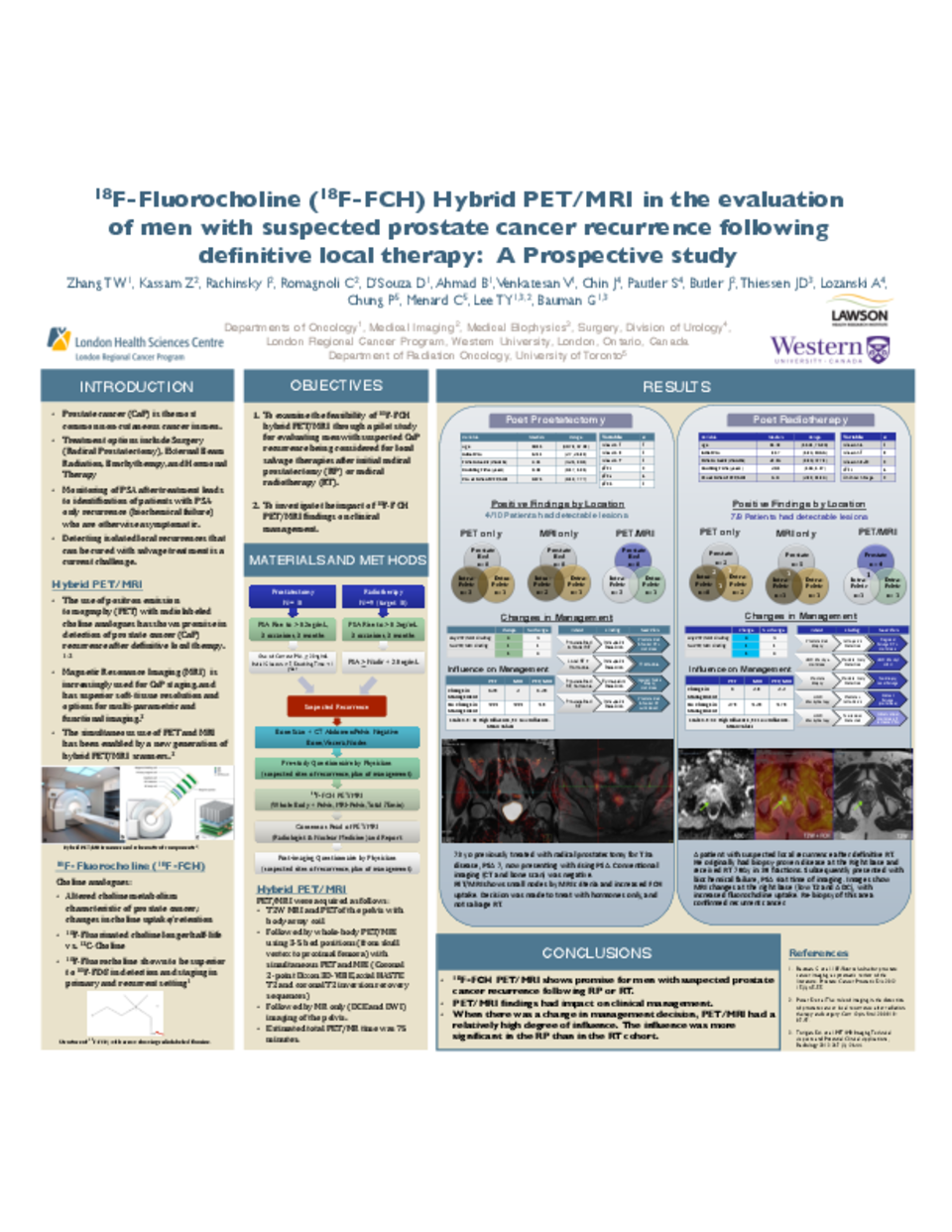
Introduction:Positron emission tomography (PET) with radiolabeled choline analogues has shown promise in detection of prostate cancer (CaP) recurrence after definitive local therapy.1-2 Magnetic Resonance Imaging (MRI) is increasingly used for CaP staging, and has superior soft-tissue resolution and options for multi-parametric and functional imaging.3 The simultaneous use of PET and MRI has been enabled by a new generation of hybrid PET/MRI scanners. 3 We designed a pilot study examining the feasibility of hybrid PET/MRI using 18F-FCH for evaluating men with suspected CaP recurrence who were being considered for local salvage therapies after initial radical prostatectomy (RP) or radical radiotherapy (RT).
Materials and Methods: Nineteen men with suspected CaP recurrence and negative conventional restaging (bone scan and computed tomography) being considered for local salvage were accrued: 10 post-RP and 9 post-RT. PET/MRI were acquired as follows: T2W MRI and PET of the pelvis with body-array coil followed by whole-body PET/MRI using 3-5 bed positions (from skull vertex to proximal femora) with simultaneous PET and MRI (Coronal 2-point Dixon 3D-VIBE, axial HASTE T2 and coronal T2 inversion recovery sequences) followed by MR only (DCE and DWI) imaging of the pelvis. A PET/MRI consensus report was generated by joint read by a radiologist and nuclear medicine physician. Questionnaires were completed by the referring physicians prior to and after imaging reports to investigate the clinical impact of PET/MRI.
Results :Median PSA of the 10 post-RP men at the time of PET/MRI imaging was 0.575 (range 0.19-7.77). Seven men had initial Gleason Scores (GS) of 7, and two had GS 8-9. One had no GS available due to prior hormonal effects. Four of 10 post-RP men had lesions detected on PET/MRI; 3 in pelvic nodes and 1 in distant nodes. Most had concordant PET and MRI findings. Change in management occurred in 100% (4/4) with positive PET/MRI and 0/6 with negative PET/MRI. The Influence of PET/MRI on change in management was scored a mean of 1.25 by physicians in questionnaires (scale of 1-5, 1 being high influence). Median PSA of the 9 post-RT men at the time of PET/MRI was 6.0 (range 2.89-11.84). Eight men had initial GS of 7, and 1 had GS 6. Seven of 9 men had lesions detected on PET/MRI; 4 isolated to the prostate, 1 in the prostate and pelvic nodes, 1 in pelvic nodes, and 1 distant. Concordance between PET/MRI findings was less than in the RP cohort. Change in management occurred in 57% (4/7) with positive PET/MRI and 1/2 with negative PET/MRI. The Influence of PET/MRI on change in management was scored a mean of 2.2 by physicians.
Conclusions: 18F-FCH PET/MRI shows promise for men with suspected CaP recurrence following RP or RT. PET/MRI findings had impact on clinical certainty of sites of recurrence and management.
1.Prostate Cancer Prostatic Dis. 2012 15(1):45-55. 2.Curr Opin Urol. 2008 18: 87-97. 3.Radiology 2013 267 (1): 26-44.



