Abstract
Purpose: To compare disease free survival (DFS) rates using a >0.4ng/mL biochemical failure definition with the Phoenix (nadir+2ng/mL) failure definition using a consecutive cohort of 1006 patients treated with dose rate brachytherapy (LDR-PB) monotherapy.
Materials and Methods: Data for 1006 consecutive LDR-PB implants (1998 to 2003) were extracted from a prospective database. Patients had low (58%) or intermediate (42%) risk disease. Adjuvant androgen deprivation therapy (ADT) was used in 65% of cases.
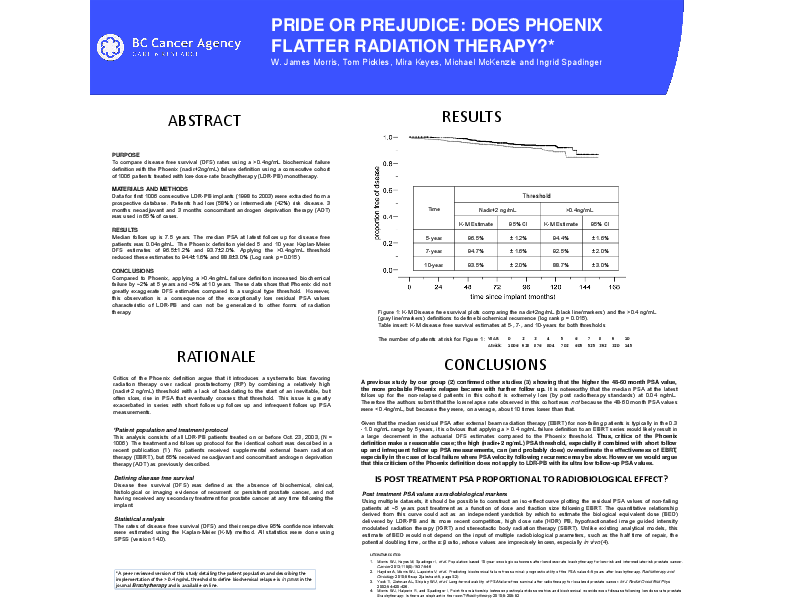
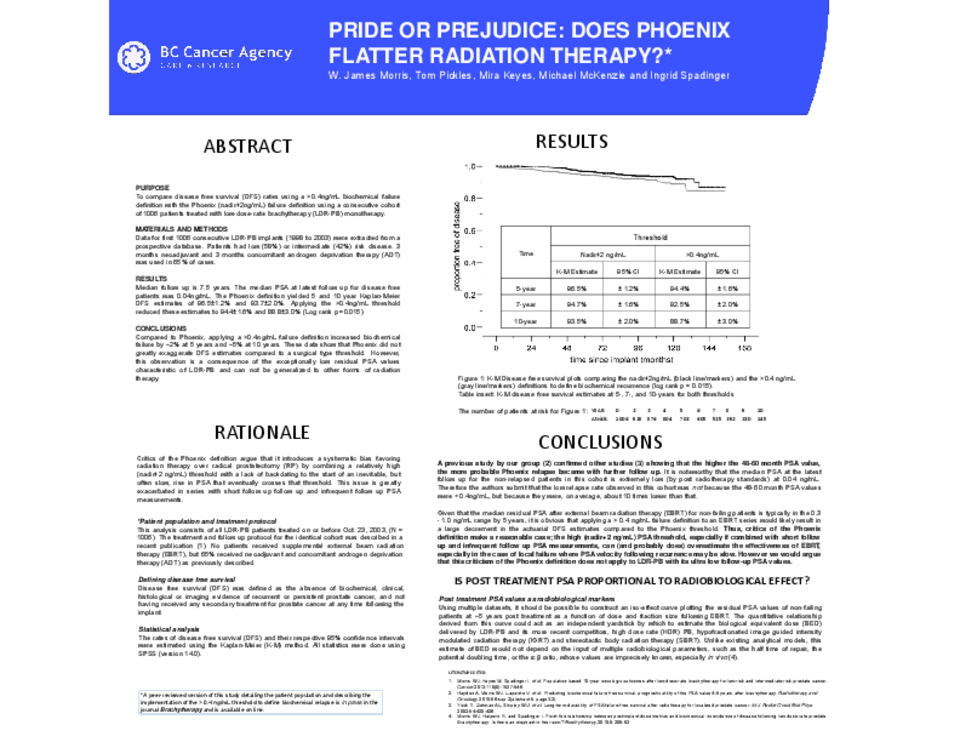
Results: Median follow-up is 7.5 years. The median PSA at latest follow-up for disease free patients was 0.04ng/mL. The Phoenix definition yielded five- and 10-year Kaplan-Meier DFS estimates of 96.5±1.2% and 93.7±2.0%. Applying the >0.4ng/mL threshold reduced these estimates to 94.4±1.6% and 88.8±3.0% (Log rank p=0.012).
Conclusions: Compared to Phoenix, applying a >0.4ng/mL failure definition increased biochemical failure by ~2% at five years and ~5% at 10 years. These data show that Phoenix did not greatly exaggerate DFS estimates compared to a surgical type threshold. However, this observation is a consequence of the exceptionally low residual PSA values characteristic of LDR-PB and cannot be generalized to other forms of radiation therapy.