Abstract
Stacey Yemchuk, Sandeep Dhaliwal, Anthony Nichols, John Yoo, Nancy Read, Kevin Fung, Varagur Venkatesan, Alex Hammond, Andrew Warner, John Barrett, David Palma
University of Western Ontario, London, ON, Canada
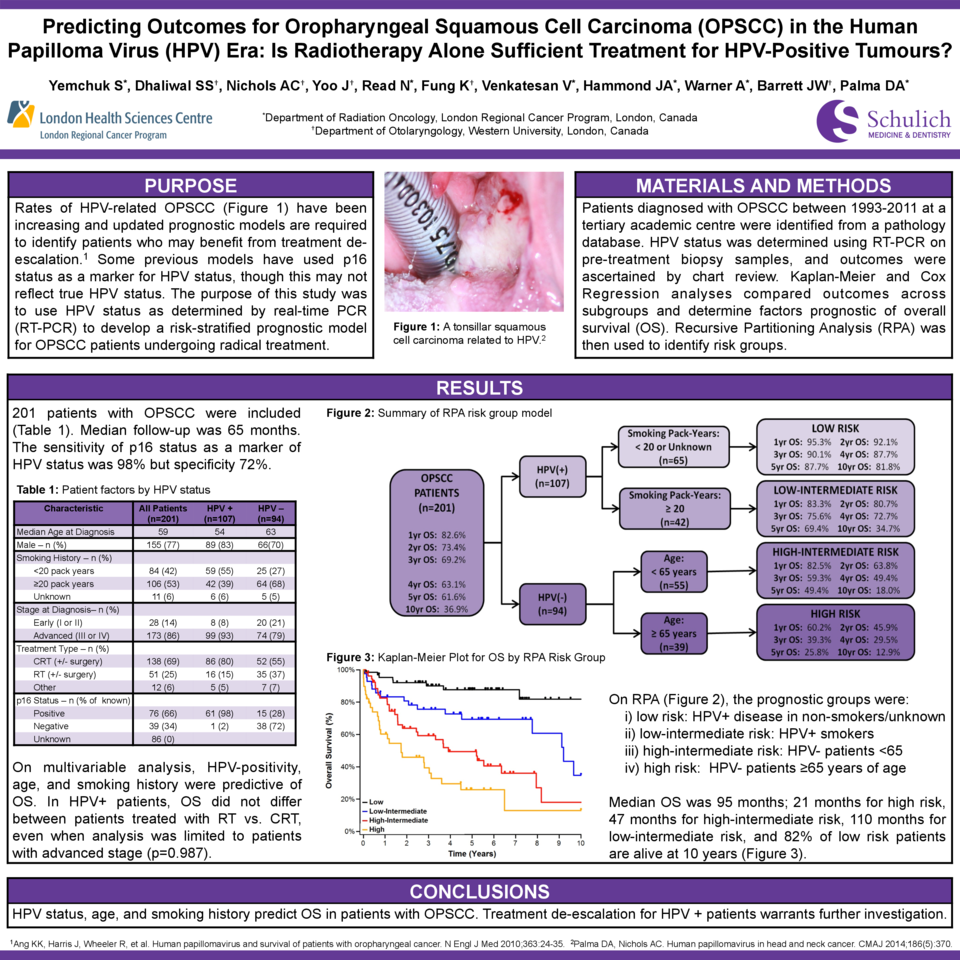
Purpose: Rates of HPV-related OPSCC have increased in Canada over the past decade. Updated prognostic models are required to inform prognosis and identify patients who may benefit from treatment de-escalation. Some previous prognostic models have used p16 status as a surrogate marker for tumour HPV status, although p16 status may not reflect true HPV status. The goal of this study was to use HPV status, as determined by real-time polymerase chain reaction (PCR), to develop a prognostic model for patients with OPSCC undergoing radical treatment.
Materials and Methods: Patients diagnosed with OPSCC between 1993-2011 at a tertiary academic centre were identified from a pathology database. HPV status was determined using real-time PCR on pre-treatment primary biopsy samples, and outcomes were ascertained by chart review. Kaplan-Meier and Cox Regression analyses were used to compare outcomes across subgroups and determine factors prognostic of overall survival (OS). Recursive Partitioning Analysis (RPA) was then used to identify risk groups.
Results: Two hundred and two patients with OPSCC met the inclusion criteria. Median follow-up was 65 months. Median age was 58 years (range 23-94), 156 patients (77%) were male, and most had Stage III (33; 16%) or Stage IV (141; 70%) disease. p16 status was available for 115 patients (57%), of which 76 patients (66% of those tested) were p16-positive. HPV PCR status was available for all patients and 107 (53%) were positive; 98% for HPV-16. The sensitivity of p16 status as a surrogate marker of HPV status was excellent (98.4%) but specificity was modest (71.7%). Treatments consisted of primary radiotherapy (RT, 23%), chemoradiotherapy (CRT, 58%), induction chemotherapy followed by CRT (7%), and surgical resection or other (12%). Median OS of all patients was 95 months; OS was 134 months for HPV+ patients versus 36 months for HPV– patients (p<0.001). On multivariable analysis, factors predictive of OS were HPV-positivity (HR=0.35, p<0.001), increasing age (HR=1.04 per year, p=0.001), and smoking history (HR=1.57, p=0.016). In HPV+ patients, OS did not differ between patients treated with RT versus CRT (p=0.826), even when the analysis was limited to patients with advanced stage. Five-year OS for HPV+ patients treated with RT alone was 84%. On RPA, the major prognostic groups identified were: 1) HPV+ disease in non-smokers (five-year OS 88%); 2) HPV+ disease in smokers (five-year OS 70%); 3) HPV– disease in young patients ≤70 years of age (five-year OS 47%); and 4) HPV- disease in patients >70 years of age (five-year OS 19%).
Conclusions: In OPSCC, factors predictive of OS include HPV status, age, and smoking history. HPV status is best determined using real-time PCR, as p16 status as a surrogate maker has only modest specificity. Treatment de-escalation for HPV+ patients warrants further investigation.