Abstract
Alireza Fotouhi Ghiam, Harald Keller, Michael Sharpe, Barbara-Ann Millar, Peter Chung, David Jaffray, Arjun Sahgal, Daniel Létourneau
University of Toronto, Toronto, ON
Purpose: Rotational setup errors are often observed for spine SBRT patients, but their dosimetric impact has been difficult to assess and, therefore, tolerance thresholds for repositioning have been somewhat arbitrary. We performed an automated planning study to estimate the dosimetric impact of rotational setup errors on cord dose for spine SBRT patients and determine potential predictors for spinal cord dose sensitivity to rotational errors.
Materials and Methods: Seventeen patients with spinal metastasis treated with spine SBRT (18 Gy/1 fraction) were identified and nine-field IMRT plans were generated. The intent was to maximize target coverage while maintaining the maximum 0.1cc spinal cord dose (Dcord) to 10 Gy. The maximum dose to 0.1cc of the volume consisting of the cord + 2mm margin (DPRV2) was recorded. Rotational setup errors alone (combination 0-12° around X, Y and Z axis) and in combination with 1mm translational setup errors along the X and Y axes were introduced alternatively in each patient’s CT dataset and the treatment planning system was used in a batch mode to compute the dosimetric impact on the spinal cord. Rotational setup errors were considered non-negligible if Dcord reached or exceeded the original DPRV2. Rotation combinations around the three different axes were reduced to a single equivalent rotation angle (qeq) around an arbitrary axis using eigenvector formalism, and the minimum qeq for which Dcord = DPRV2 was compiled. Dimensions of the dose distributions and its location with respect to the cord were evaluated as predictive factors for Dcord sensitivity to rotational errors using regression analysis.
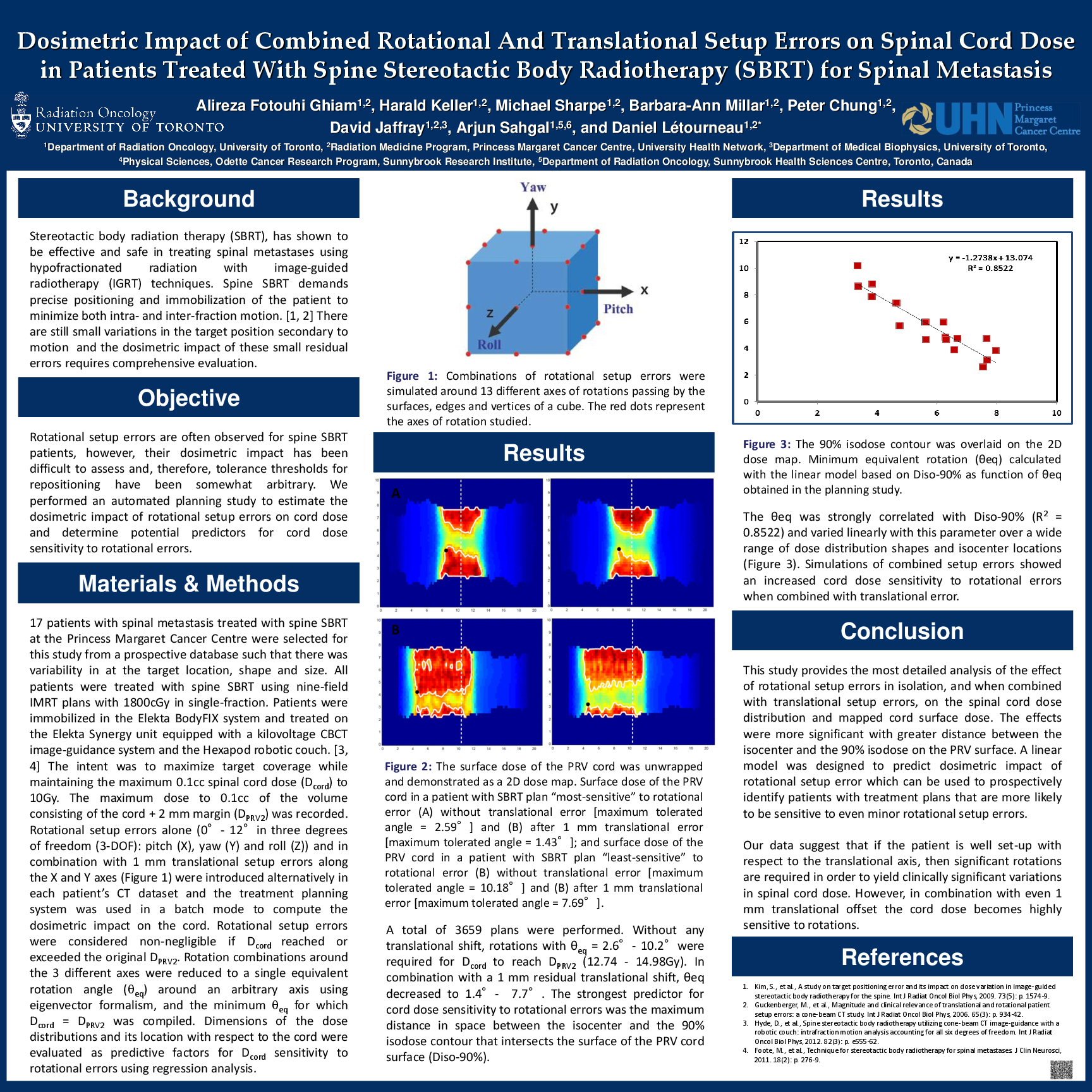
Results: A total of 3659 plans were performed. Without any translational shift, rotations with θeq=2.6°-10.2° were required for Dcord to reach DPRV2 (12.74-14.98Gy). In combination with a 1mm residual translational shift, θeq decreased to 1.4°-7.7°. The strongest predictor for cord dose sensitivity to rotational errors was the maximum distance in space between the isocenter and the 90% isodose contour that intersects the surface of the PRV cord surface (Diso-90%). The θeq was strongly correlated with Diso-90% (R2=0.8522) and varied linearly with this parameter over a wide range of dose distribution shapes and isocenter locations. Simulations of combined setup errors showed an increased cord dose sensitivity to rotational errors when combined with translational error.
Conclusions: This study provides the most detailed analysis of the effect of rotational setup errors in isolation, and when combined with translational setup errors, on the spinal cord dose distribution and mapped cord surface dose. The effects were more significant with greater distance between the isocenter and the 90% isodose on the PRV surface. A linear model was designed to predict dosimetric impact of rotational setup error which can be used to prospectively identify patients with treatment plans that are more likely to be sensitive to even minor rotational setup errors.