Abstract
Jessica Conway1, Ivo Olivotto1, Stacy Miller2, Ross Halperin3, David Hoegler3, Wayne Beckham4, Joanne Stephen5, Helena Daudt4, John French1, Rob Olson2
1British Columbia Cancer Agency, Vancouver, BC
2British Columbia Cancer Agency, Centre for the North, Prince George, BC
3British Columbia Cancer Agency, Centre for the Southern Interior, Kelowna, BC
4British Columbia Cancer Agency, Vancouver Island Cancer Centre, Victoria, BC
5British Columbia Cancer Agency, Fraser Valley Cancer Centre, Surrey, BC
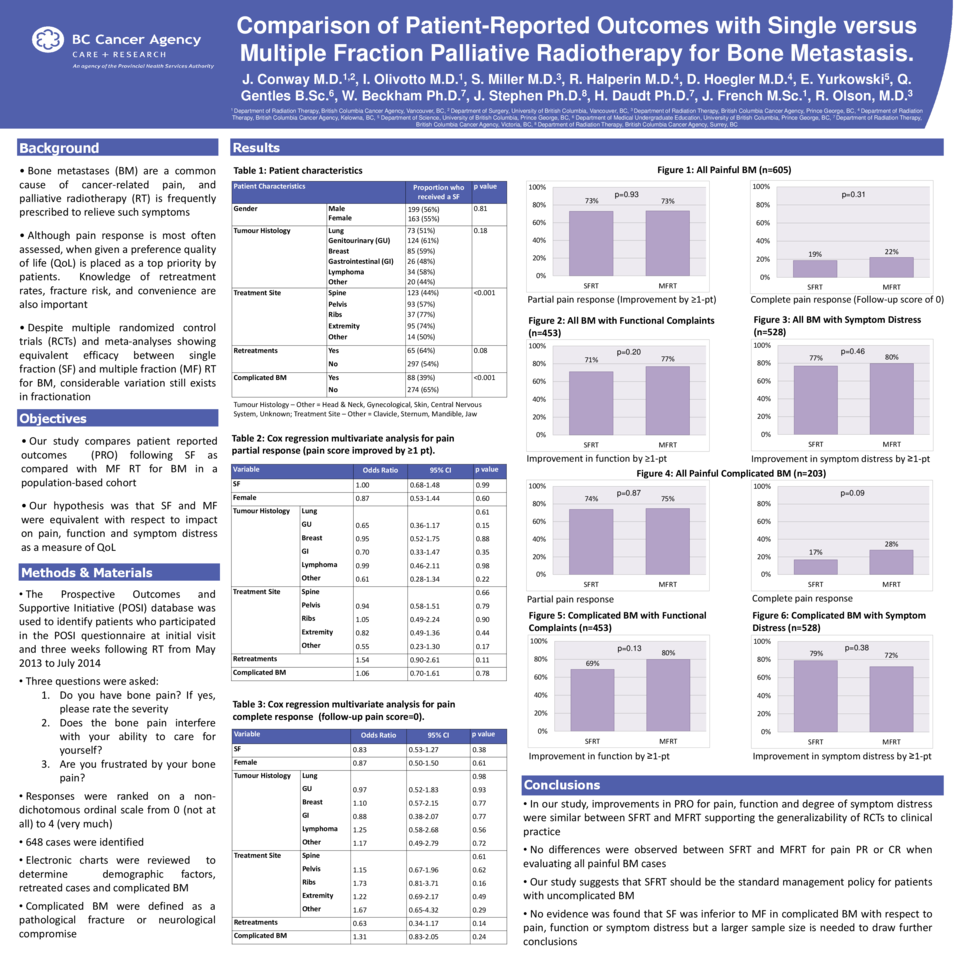
Purpose: To compare patient reported outcomes (PROs) following single fraction (SF) as compared with multiple fraction (MF) radiation therapy (RT) for uncomplicated bone metastases in a population-based cohort.
Materials and Methods: Six British Columbia Cancer Agency centres participated in the Prospective Outcomes and Support Initiative (POSI), to record PROs prior to and three weeks following RT for uncomplicated bone metastases. Patients treated in BC between May and December 2013 who provided PROs before and after RT were identified. PROs were standardized and designed to assess patients’ perception of pain, function and symptom distress using a non-dichotomous, ordinal, 5-point scale. Comparisons were made between patients who received SF versus MF RT. SFRT versus MFRT was at the discretion of the treating oncologist. A multivariate logistic regression analysis was performed.
Results: Two hundred and eighty-four patients completed both pre- and post-RT assessments. The mean age at diagnosis was 64 years, 50% were male, and 59% received SFRT. The three most common primary sites were genitourinary (29%), lung (24%) and breast (20%). Spine (47%) was the most common site treated. There were no significant differences in changes in mean PRO scores for pain (1.17 versus 1.02 point improvement; p=0.74), function (0.74 versus 0.82 point improvement; p=0.61) or degree of symptom distress (1.22 versus 1.21 point improvement; p=0.94) between patients who received SFRT versus MFRT. Likewise, the proportion of patients with at least a 1-point improvement in pain (68.2% versus 70.0%; p=0.78), function (73.2% versus 66.7%; p=0.41), and distress (78.5% versus 80.7%; p=0.74) were similar between SFRT and MFRT. After controlling for age at diagnosis, gender, fractionation, site of delivery, and disease site there was no significant difference in probability of having an improvement in at least one category between SFRT and MFRT (Odds Ratio=1.43; 95% CI 0.76-2.68; p=0.27).
Conclusions: Improvements in patients’ pain, function and degree of distress were similar whether treated with SFRT or MFRT. These population-based data support the generalizability of the randomized controlled trials to real-world practice and confirm that SFRT should be the standard management policy for patients with uncomplicated bone metastases



