Abstract
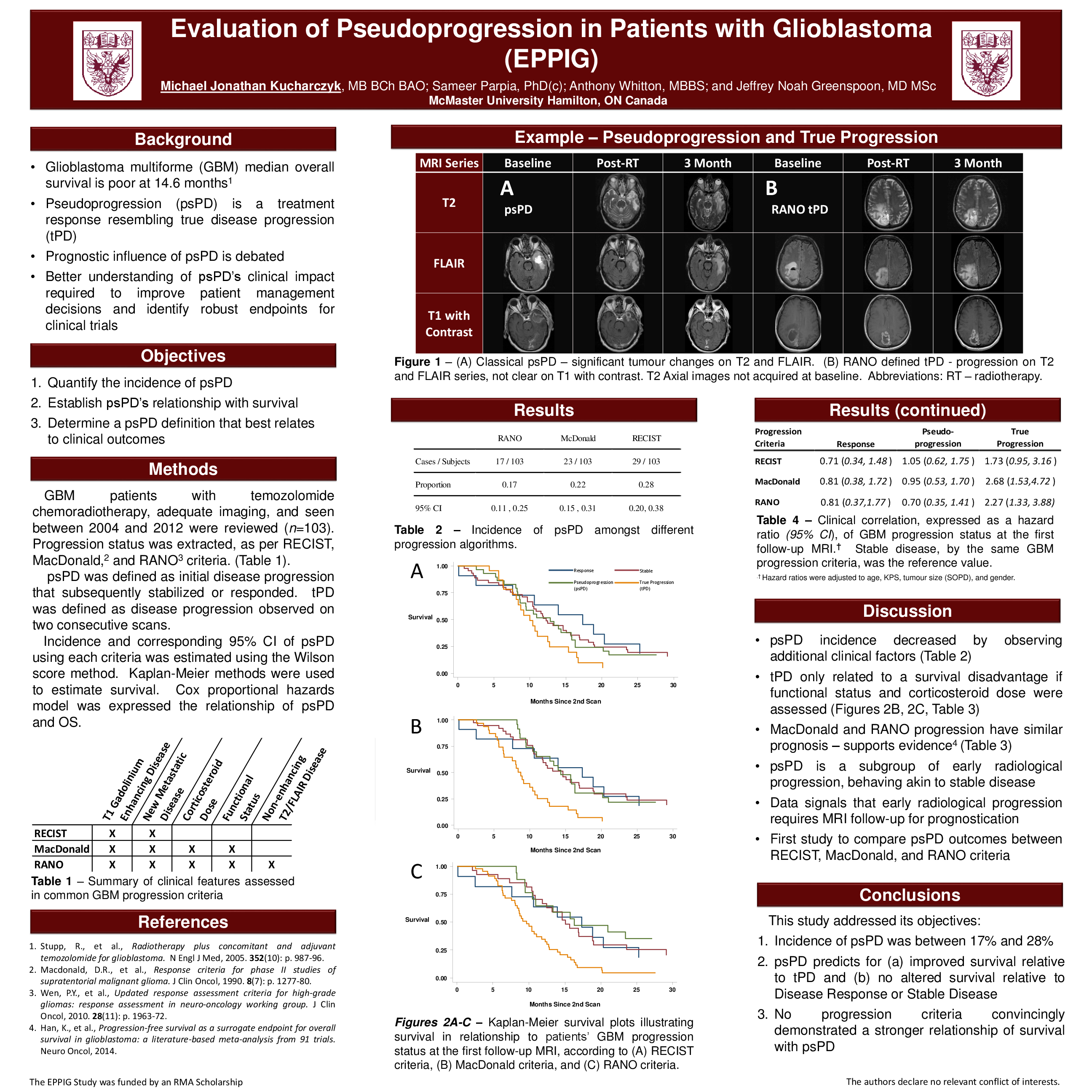
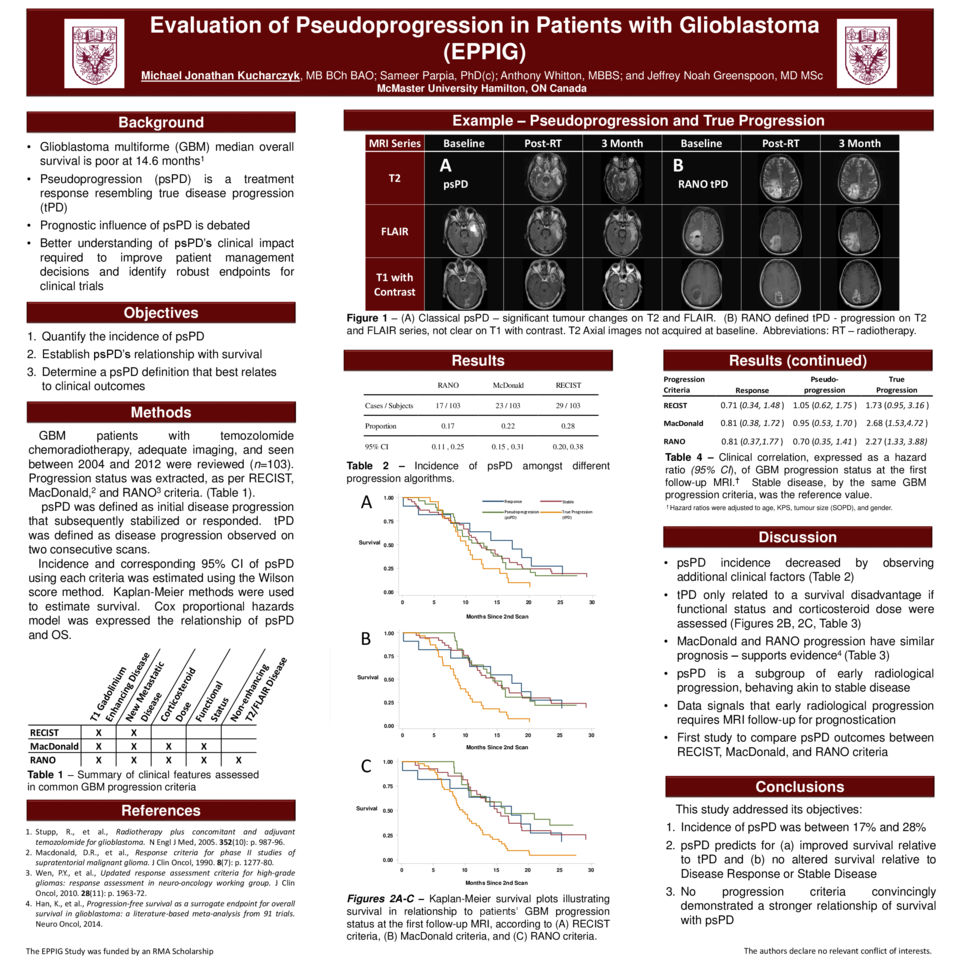
Background: Management of glioblastoma (GBM) is complicated by pseudoprogression (psPD), a radiological phenomenon mimicking progression. This retrospective study investigated the incidence, prognostic implications, and most clinically appropriate definition of psPD.
Method: Patients seen between 2004 and 2012 at a neuro-oncology multidisciplinary clinic were subject to a chart review (n=362). GBM patients treated with temozolomide chemoradiotherapy and with adequate imaging - contrast-enhanced magnetic resonance imaging (MRI) prior to treatment, within 12 weeks of treatment, and at next follow-up - were included (n=100). At each MRI, the RECIST, MacDonald, and Response Assessment in Neuro-Oncology (RANO) status were reported. Statistical analysis contrasted survival to disease response (DR), stable disease (SD), psPD, and true progression (tPD).
Results: psPD incidence was 17% (95% CI, 11-25%), 22% (95% CI, 15-31%) and 28% (95% CI, 20-38%), as defined by RANO, MacDonald, and RECIST criteria, respectively. Observing RANO and MacDonald definitions, similar survival was appreciated with psPD (hazard ratio [HR] 0.70; 95% CI, 0.35-1.41 and HR 0.95; 95% CI, 0.53-1.70) and DR (HR 0.81; 95% CI, 0.37-1.77 and HR 0.81; 95% CI, 0.38-1.72), compared to SD. tPD relative to SD, as defined by RANO and MacDonald, was associated with impaired survival (HR 2.27; 95% CI, 1.33-3.88 and HR 2.68; 95% CI, 1.53-4.72). RECIST evaluation indicating DR (HR 0.71; 95% CI, 0.34-1.48), psPD (HR 1.05; 95% CI, 0.62-1.75), or tPD (HR 1.73; 95% CI 0.95-3.16) were not statistically distinguishable from SD.
Conclusions: By evaluating progression of GBM by conventional methods, RANO-defined psPD minimized psPD incidence and had the strongest indication of improved survival.