Abstract
Purpose
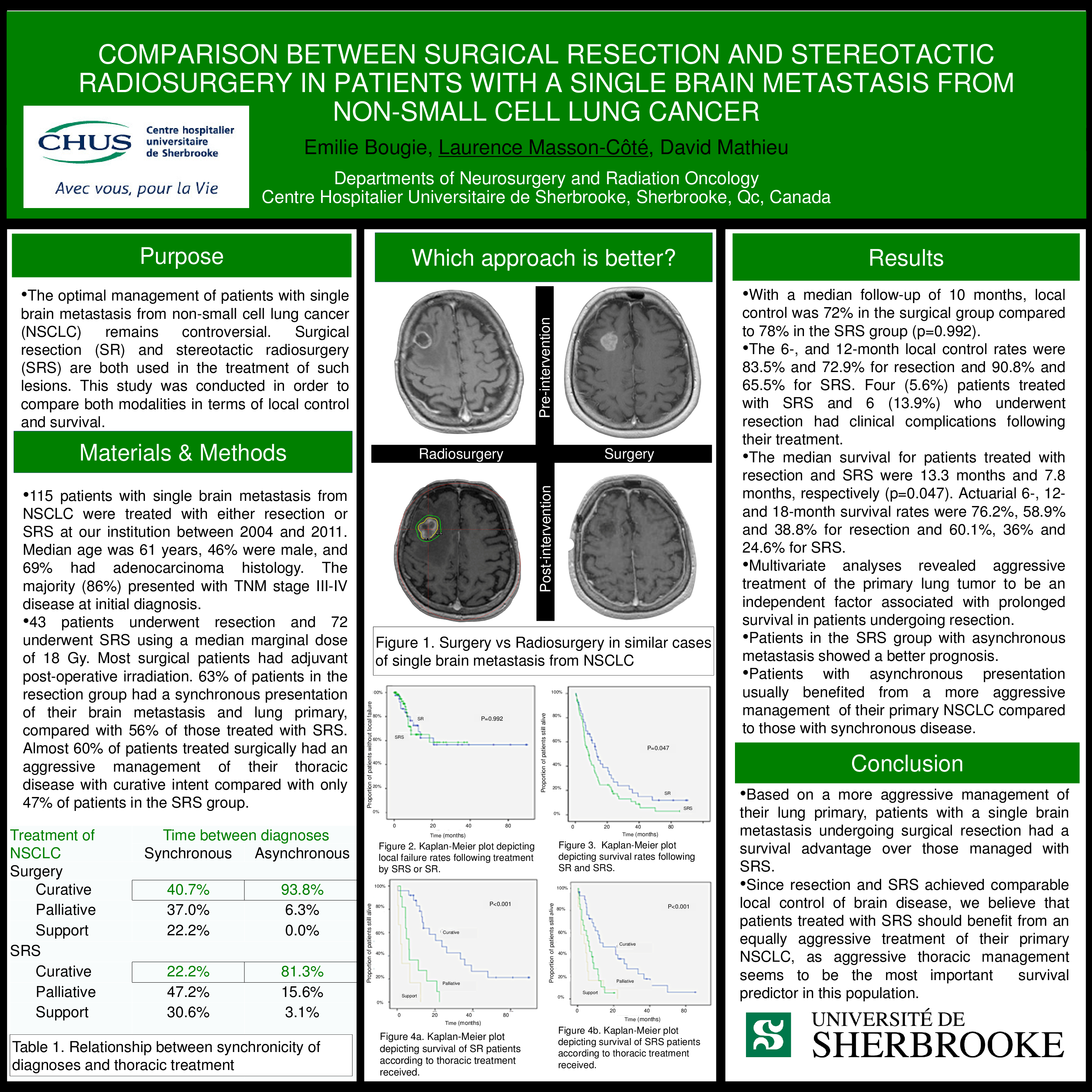
•The optimal management of patients with single brain metastasis from non-small cell lung cancer (NSCLC) remains controversial. Surgical resection (SR) and stereotactic radiosurgery (SRS) are both used in the treatment of such lesions. This study was conducted in order to compare both modalities in terms of local control and survival.
Materials & Methods
•115 patients with single brain metastasis from NSCLC were treated with either resection or SRS at our institution between 2004 and 2011. Median age was 61 years, 46% were male, and 69% had adenocarcinoma histology. The majority (86%) presented with TNM stage III-IV disease at initial diagnosis.
•43 patients underwent resection and 72 underwent SRS using a median marginal dose of 18 Gy. Most surgical patients had adjuvant post-operative irradiation. 63% of patients in the resection group had a synchronous presentation of their brain metastasis and lung primary, compared with 56% of those treated with SRS. Almost 60% of patients treated surgically had an aggressive management of their thoracic disease with curative intent compared with only 47% of patients in the SRS group.
Results
•With a median follow-up of 10 months, local control was 72% in the surgical group compared to 78% in the SRS group (p=0.992).
•The 6-, and 12-month local control rates were 83.5% and 72.9% for resection and 90.8% and 65.5% for SRS. Four (5.6%) patients treated with SRS and 6 (13.9%) who underwent resection had clinical complications following their treatment.
•The median survival for patients treated with resection and SRS were 13.3 months and 7.8 months, respectively (p=0.047). Actuarial 6-, 12- and 18-month survival rates were 76.2%, 58.9% and 38.8% for resection and 60.1%, 36% and 24.6% for SRS.
•Multivariate analyses revealed aggressive treatment of the primary lung tumor to be an independent factor associated with prolonged survival in patients undergoing resection.
•Patients in the SRS group with asynchronous metastasis showed a better prognosis.
•Patients with asynchronous presentation usually benefited from a more aggressive management of their primary NSCLC compared to those with synchronous disease.
Conclusion
•Based on a more aggressive management of their lung primary, patients with a single brain metastasis undergoing surgical resection had a survival advantage over those managed with SRS.
•Since resection and SRS achieved comparable local control of brain disease, we believe that patients treated with SRS should benefit from an equally aggressive treatment of their primary NSCLC, as aggressive thoracic management seems to be the most important survival predictor in this population.