Abstract
Authors
Kenneth McKinley, Shanu Kurd, William Schweickert, Megan Carr-Lettieri, Marybeth O’Malley, Shahid Sulaiman, Jennifer Myers
Institutions
Medicine, Hospital of the University of Pennsylvania
Raymond and Ruth School of Medicine at the University of Pennsylvania
Purpose of Study
Wrong-site, wrong-procedure and wrong-patient errors occur despite regulatory requirements that Universal Protocol, or a pre-procedure “time-out” (TO), be performed before every invasive procedure. Although the initial emphasis on Universal Protocol was in the operating room, a significant proportion of these errors occur during bedside procedures. Little is known about the rigor of this practice in the non-operative setting.
Methods Used
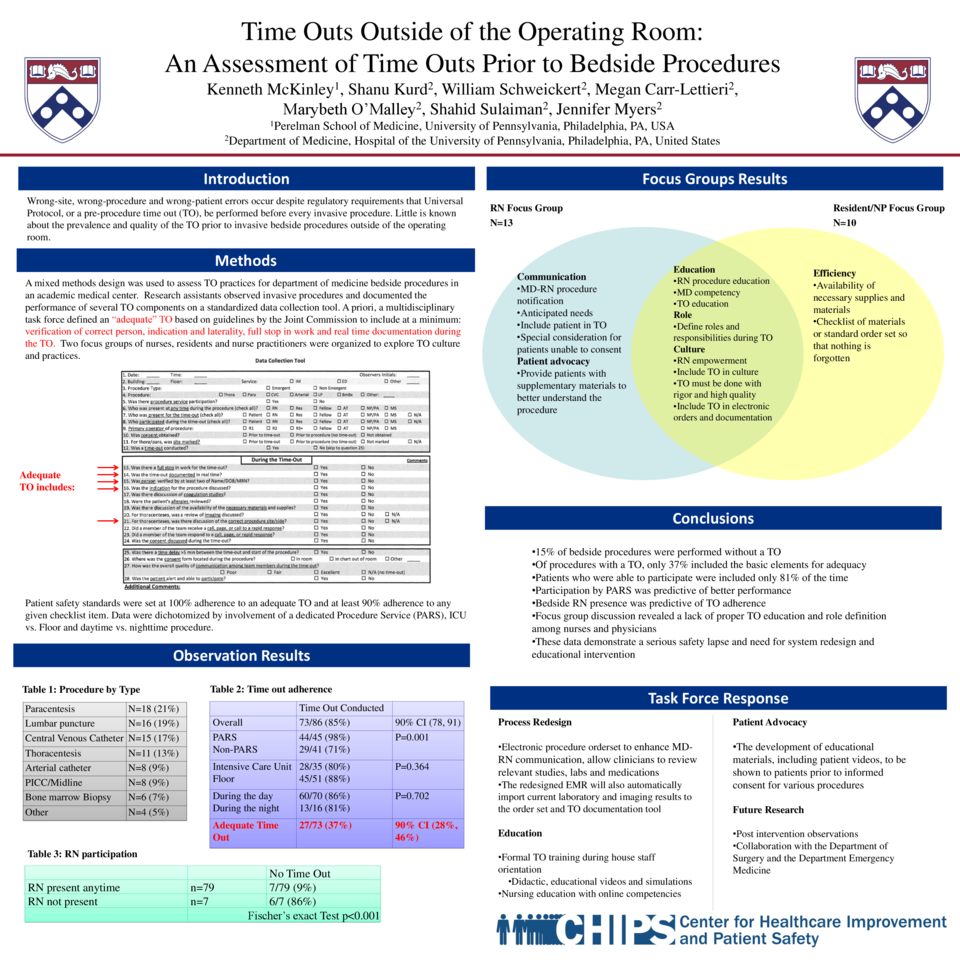
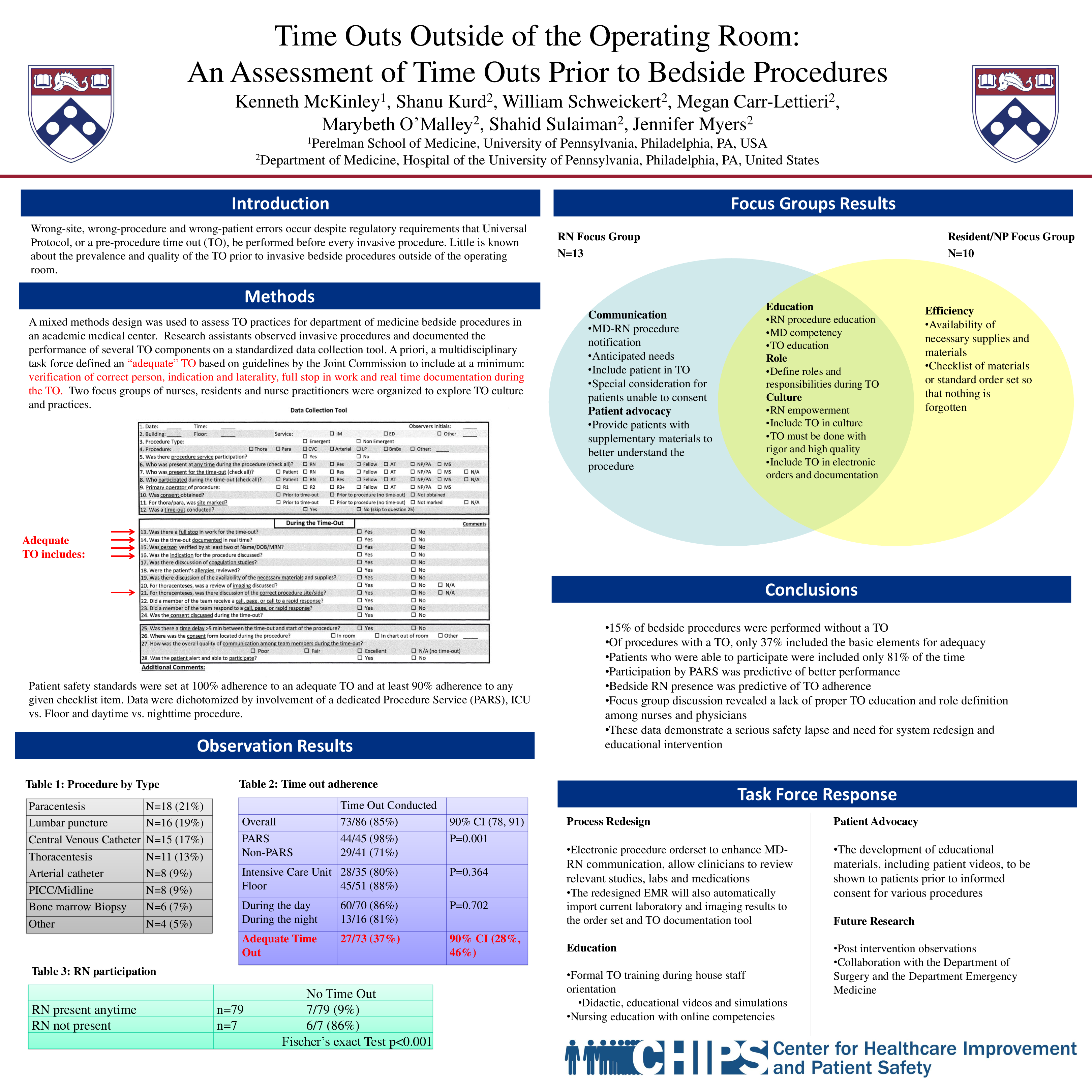
A mixed methods design was used to assess TO practices for internal medicine bedside procedures in an academic medical center. Research assistants observed invasive procedures and documented the performance of several TO components on a standardized data collection tool. A priori, a multidisciplinary task force defined a “high quality” TO to include verification of correct person, indication and laterality, as well as a full stop in work and real time documentation during the TO. Other items included a review of imaging, nurse participation, and discussion of allergies, consent and supplies. Two focus groups of nurses, residents and nurse practitioners were organized to consider TO culture and practices.
Summary of Results
Eighty-six procedures were observed: 52% performed by a dedicated procedure service, 81% performed during the day and 41% in an ICU. A TO was performed prior to 85% (90% CI: 78, 91). Procedure service participation was predictive of TO adherence (p=0.001) and inclusion of more checklist items (p<0.001), whereas procedures performed during the day (p=0.702) or in the ICU (p=0.364) were not. Only 37% (90% CI: 28, 46) of TOs met criteria for high quality. Focus groups identified patient and nurse procedure education, availability of supplies, improved clarification of clinician roles and physician-nurse communication around procedure scheduling as potential areas for improvement.
Conclusions
Non-operative bedside procedures are a vulnerable setting for wrong-site, wrong-procedure and wrong-patient errors due to inadequate time-outs. Efforts should be made to standardize all aspects of the time-out process with an emphasis on time-out content, interdisciplinary communication and role clarification to eliminate preventable medical errors.