Is there an optimum location to measure non-invasive blood pressure in morbidly obese patients?
Abstract
Objective:
In morbidly obese patients, oscillometric blood pressure measured with an upper-arm blood pressure cuff may be difficult to perform due to the size and shape of the arm1. In addition, the value of the measurements obtained may be questionable2. An alternative method is invasive blood pressure monitoring using an arterial catheter, but these can be difficult to place and are associated with risks3. Currently there are no recommendations for the optimal location of an oscillometric blood pressure cuff in the morbidly obese. We compared the reliability of blood pressure readings obtained with an oscillometric device using various cuff placements and wrapping techniques with those obtained by intra-arterial measurement in morbidly obese patients.
Methods:
Sixteen morbidly obese patients ASA class I, II, and III undergoing non-cardiac surgery were enrolled. Intraoperative blood pressure was simultaneously measured using an oscillometric blood pressure cuff and an arterial catheter placed in the ipsilateral radial artery. Oscillometric blood pressure measurements were taken with the cuff placed cylindrically and conically around the upper arm and cylindrically around the forearm. Patient BMI, proximal upper arm circumference, distal upper arm circumference, forearm circumference and blood pressure cuff size were recorded. Systolic (SBP), diastolic (DBP) and mean blood pressures (MAP) were taken twice at each oscillometric cuff location and corresponding radial arterial catheter measurements were recorded. We defined a radial artery catheter and oscillometric cuff difference of 10 mmHg to be clinically and statistically significant. Precision and bias were measured using Bland-Altman plots. Linear regression was used to describe the relationship between arm circumference and blood pressure difference. Analysis of variance followed by the T-test was used to determine between group differences in bias.
Results:
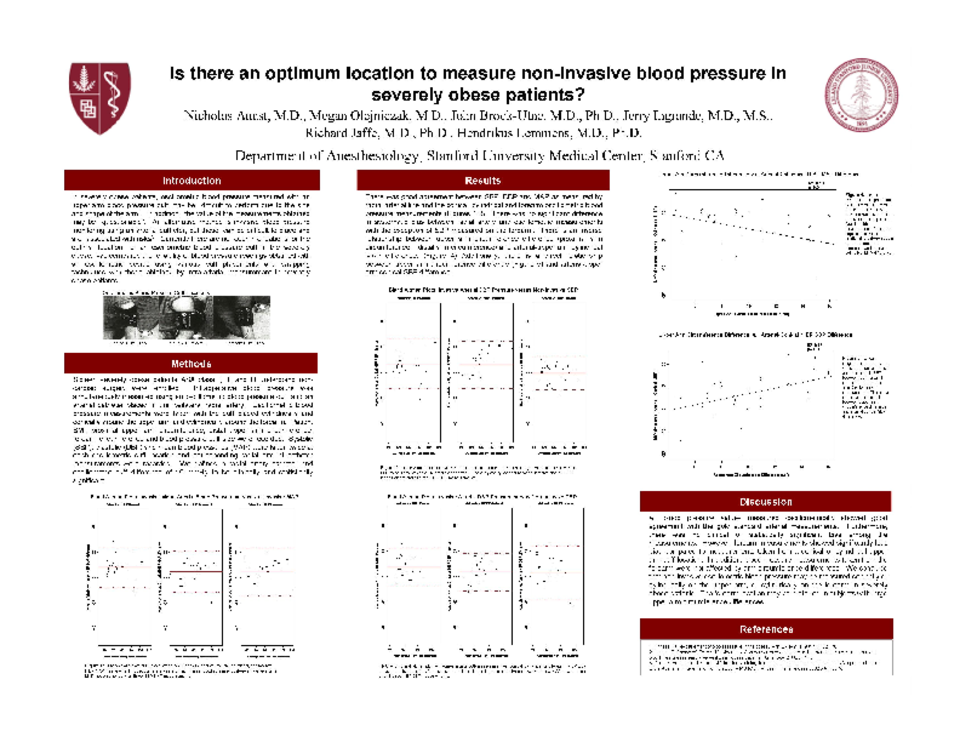
There was good agreement between SBP, DBP and MAP as measured by radial arterial line and the conical, cylindrical and forearm oscillometric blood pressure measurements (Figures 1-3). There was no significant difference in systematic bias between radial artery and oscillometric measurements with the exception of SBP measured on the forearm. There is an inverse relationship between upper arm circumference difference (proximal arm circumference – distal arm circumference) and arterial-upper arm cylindrical MAP difference. (Figure 4) Additionally, there is a direct relationship between upper arm circumference difference (Figure 5) and arterial-upper arm conical SBP difference.
Conclusion:
All blood pressure values measured oscillometrically showed good agreement with the gold standard arterial measurements. Furthermore, there was no clinical or statistically significant bias among the measurements. However, forearm measurements showed significantly less bias compared to measurements taken from a conical or cylindrical upper arm cuff location. In addition, blood pressure measurements taken from the forearm were not affected by arm circumference differences. We conclude that non-invasive oscillometric blood pressure may be measured conically or cylindrically on the upper arm, or cylindrically on the forearm in morbidly obese patients. The forearm location may be preferred in subjects with large upper arm circumference differences.
References
1. Prineas RJ: Measurement of blood pressure in the obese. Ann Epidemiol 1991;1(4):321-36.
2. Umana E, Ahmed W, Fraley MA, Alpert MA: Comparison of oscillometric and intraarterial systolic and diastolic blood pressures in lean, overweight, and obese patients. Angiology 2006;57:41-5
3. Durie M, Beckmann U, Gillies DM: Incidents relating to arterial cannulation as identified in 7,525 reports submitted to the Australian incident monitoring study (AIMS-ICU). Anaesth Intensive Care 2002;30(1):60-5.
Related articles