Abstract
Introduction:
Globally, herpes simplex virus type 1 (HSV-1) is the most common cause of fatal sporadic encephalitis and may account for up to thirty percent of the approximately 20,000 cases of viral encephalitis that are diagnosed in the United States each year. Rare cases of clinical relapse have been reported in the literature, predominantly in children. Among these relapses, those occurring more than three months after the initial infection are particularly scarce.
Case Presentation:
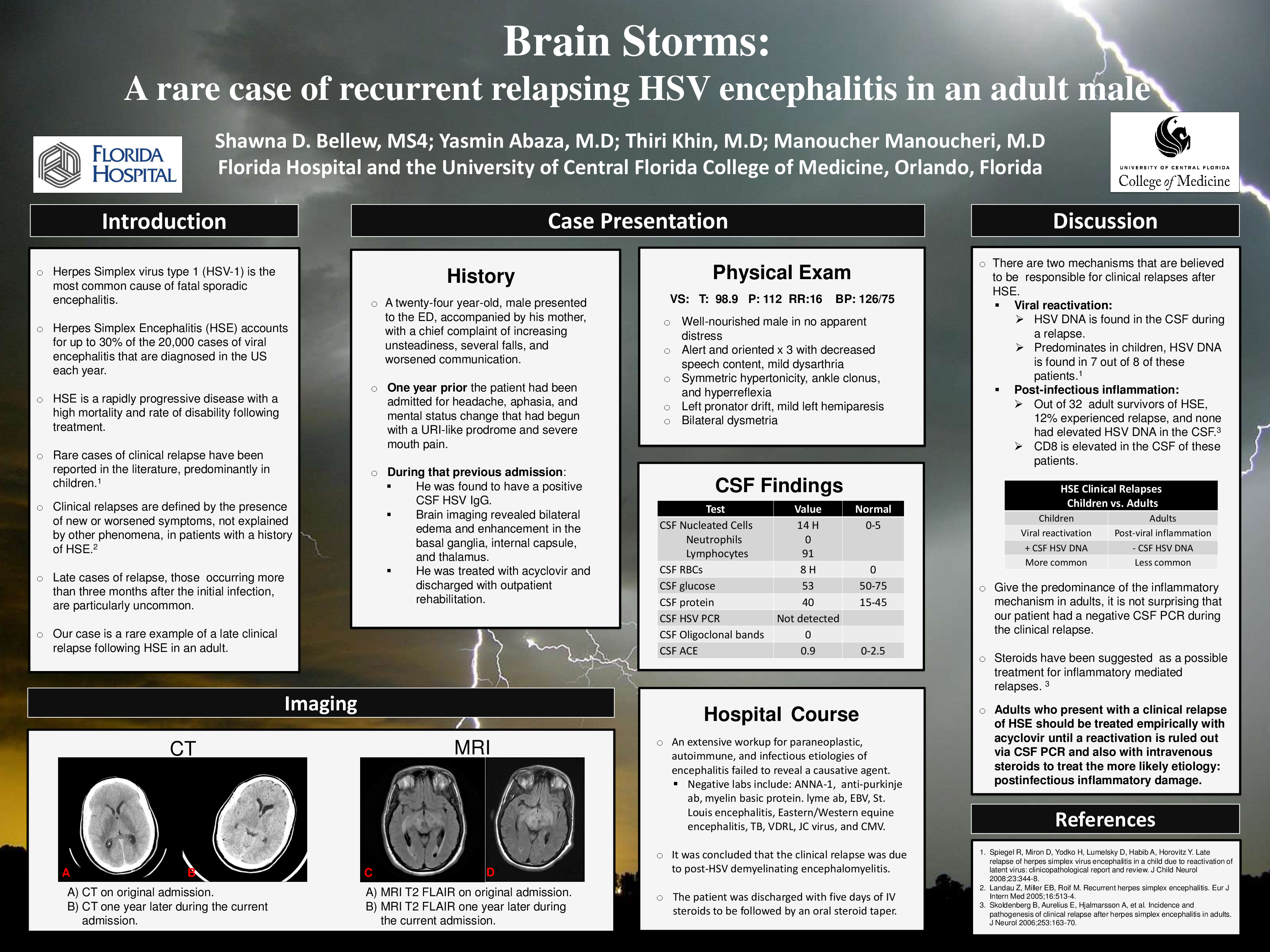
A 24-year-old man with a past medical history of neurologic deficits due to herpes simplex encephalitis (HSE) presented to the emergency department complaining of unsteadiness, several falls, and worsened communication. A year prior, the patient had been admitted to the hospital for headache, aphasia, and mental status change which had begun with a “cold”-like prodrome that included severe mouth pain. At that time, he was evaluated and found to have a positive CSF HSV IgG. Brain imaging revealed bilateral edema and signal enhancement primarily located in the basal ganglia, internal capsule, and thalamus. He was treated empirically with IV acyclovir and discharged. This admission was the third similar episode since initial presentation. On the current admission, the patient was found to be afebrile and hemodynamically stable. Physical examination was notable for an intact sensorium with decreased speech content, symmetric hypertonicity and hyperreflexia, left pronator drift, mild left hemiparesis, symmetric ankle clonus, and bilateral dysmetria. Pertinent laboratory values included CSF with lymphocytic pleocytosis. MRI of the brain revealed evidence of the earlier damage as well as new foci of increased enhancement in the left temporal lobe. An extensive workup for paraneoplastic, autoimmune, and infectious etiologies failed to reveal an agent. It was concluded that the clinical relapse was due to post-HSV demyelinating encephalomyelitis, and he was discharged with five days of IV steroids to be followed by an oral steroid taper.
Discussion:
Cases of clinical relapse after HSE are rarely reported in adults. Two mechanisms have been suggested: reactivation of the virus and postinfectious inflammation. In children, relapses are predominantly thought to be associated with reactivation of the virus, as evidenced by the presence of HSV DNA in their CSF. In adult relapses, HSV DNA is not typically found, and therefore it is thought that the damage is immune mediated. Thus, it is not surprising that the CSF HSV PCR was negative during our patient’s episodes of clinical relapse. Our case represents a rare example of late relapse of HSE. Adults with a history of HSE who present with new or worsened symptoms not explained by other phenomena should be treated empirically with acyclovir until a reactivation is ruled out via CSF PCR and also with intravenous steroids to treat the more likely etiology: postinfectious inflammatory damage.