Treating Post-Traumatic Tremor with Deep Brain Stimulation: Report of Five Cases
Abstract
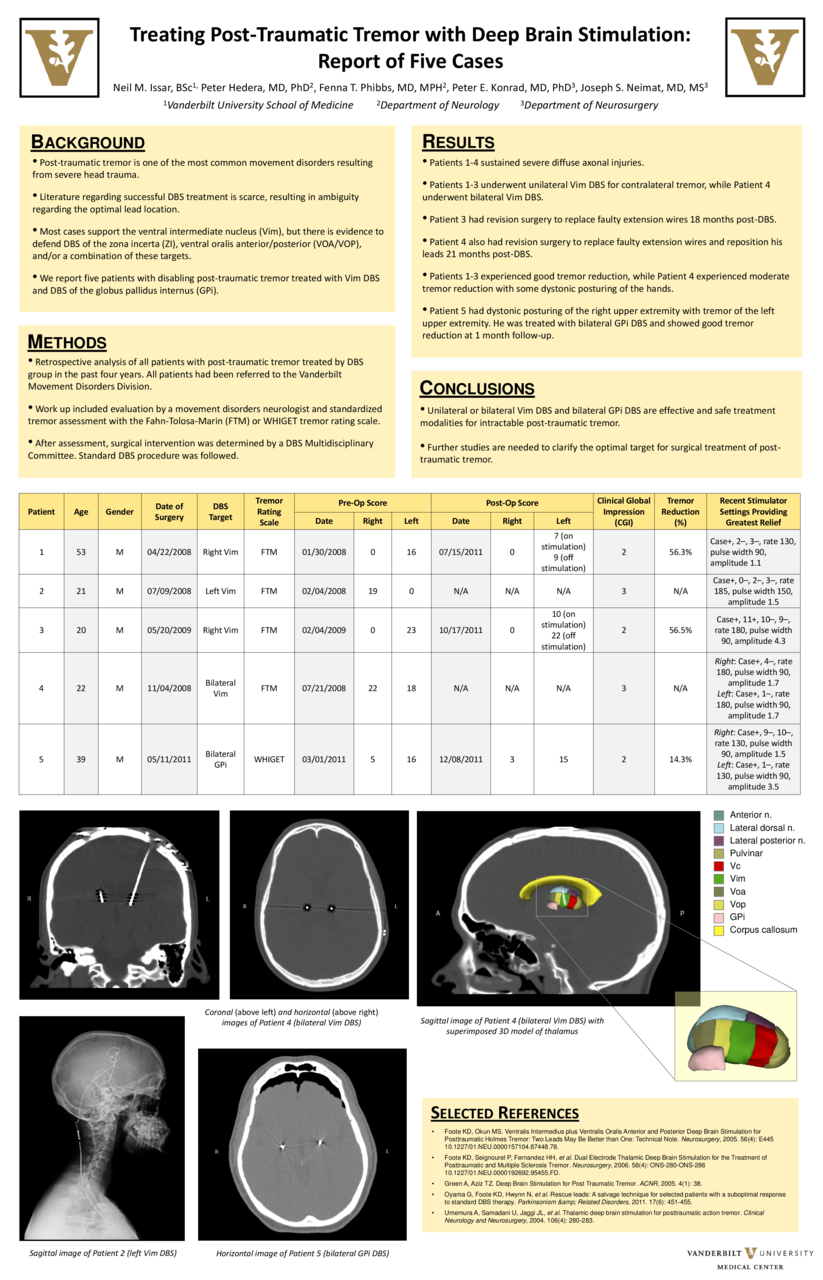
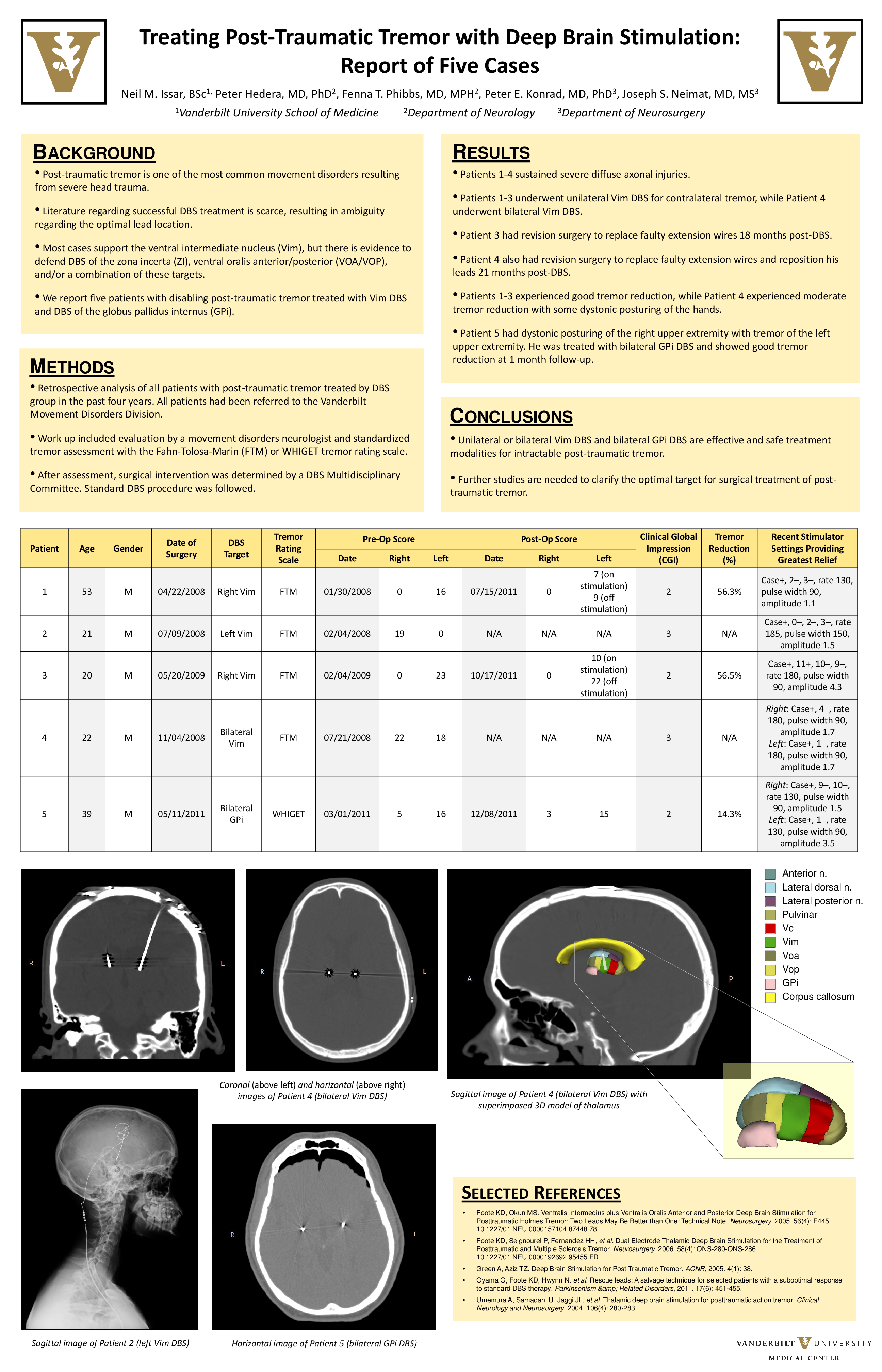
Objective: To evaluate the efficacy of deep brain stimulation in the treatment of post-traumatic tremor and to compare and discuss the role of stimulation targets including the ventral intermediate nucleus of the thalamus(VIM) and the globus pallidus internus(GPi).
Background: Post-traumatic tremor is a common complication of severe head trauma. Despite its frequency there is little literature on the treatment of post-traumatic tremor. In the past decade, deep brain stimulation (DBS) surgery has emerged as an important contributor to the care of patients with advanced tremor. However, the literature regarding post-traumatic tremor is scarce, resulting in ambiguity in target selection. There is evidence to support DBS of the VIM, GPi, zona incerta (ZI), the nucleus ventral oralis anterior/posterior (VOA/VOP), and/or a combination of these targets.
Methods: We performed a retrospective analysis of all post-traumatic tremor patients treated with DBS in the past four years. A thorough chart review was conducted. The clinical work-up for each patient included an evaluation by a movement disorders neurologist, standardized tremor assessment with the FTM or WHIGET tremor rating scale, and presentation to a multidisciplinary DBS committee where surgical intervention was determined by consensus. Standard DBS procedure was followed, including the insertion of electrode arrays with microelectrode recording and intraoperative efficacy assessment.
Results: We identified 5 patients with post-traumatic tremor that had been treated by DBS. Three patients underwent unilateral Vim DBS, one patient underwent bilateral Vim DBS, and one patient underwent bilateral GPi DBS as his tremor exhibited dystonic features. Two patients required revision surgery to replace broken extension wires. Patients undergoing both Vim and GPi stimulation achieved significant improvement in their tremor control ranging from 14.3% to 56.5% improvement in standardized tremor scale, and clinical global impression (CGI) ranging from 2 to 3.
Conclusions: DBS of the Vim and GPi is effective and safe for intractable post-traumatic tremor. The incidence of hardware complications may suggest a tendency to system failure due to incomplete tremor control. Further studies are needed to further examine this complication and to clarify the optimal target for post-traumatic tremor.
Related articles