A Model for Short-term Medical Mission Evaluation: The Impact of a Hand Surgery Mission to Honduras
Abstract
Background: Short-term medical missions—short trips to foreign countries to provide medical services to those in need—have become increasingly popular among doctors from the United States and other developed countries. It is estimated that over 6,000 such trips are coming from the United States alone to developing nations each year. Despite the large number of these trips, and the substantial resources devoted to them, little research has been published evaluating the impact of such trips on patients in a quantitative manner. With the burgeoning popularity of short-term medical missions, it is necessary to conduct quantitative outcome studies of such trips in order to develop evidence-based, comparative best practices. This study evaluates the impact of a short-term hand surgery mission to San Pedro Sula, Honduras on patient upper extremity morbidity and health-related quality of life.
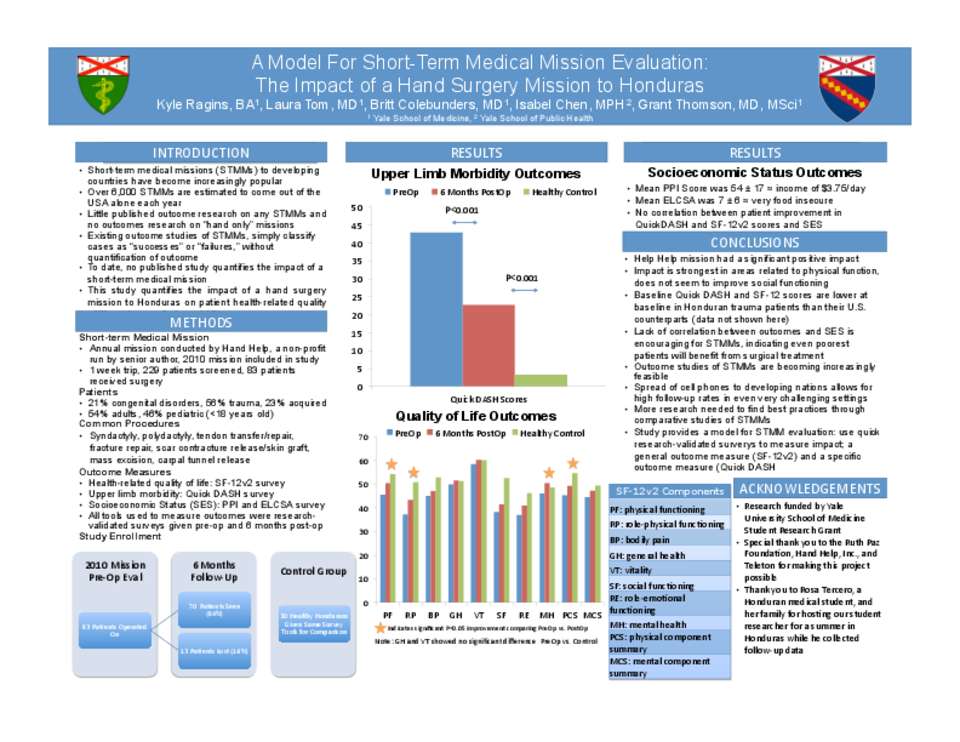
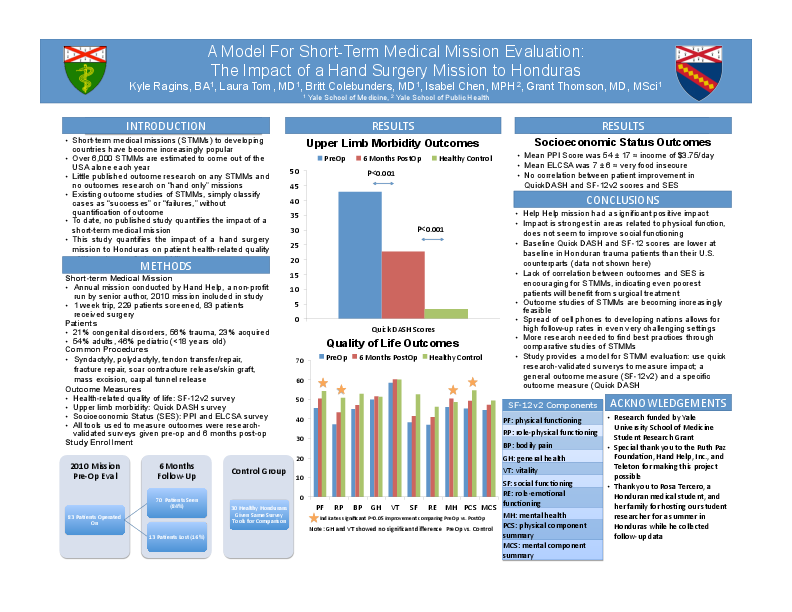
Methods: A short-term surgical mission identified Honduran patients with indications for surgery of their upper extremities and conducted surgeries on 83 patients during a weeklong trip in January 2010. Researchers administered the research-validated Quick DASH (Disability of Arm, Shoulder, and Hand) and SF-12v2 surveys preoperatively and 6 months post-operatively to patients to evaluate changes in patient upper extremity morbidity and overall health-related quality of life. In order to schedule follow-up appointments with patients 6 months post-operatively, researchers used patient mobile phones. In addition to the Quick DASH and SF-12v2, socioeconomic status data on patients was collected using both self-developed and research-validated PPI (Progress Out of Poverty Index) and ELCSA (Latin American Household Food Security Measurement Scale) surveys in order to examine socioeconomic correlations with surgical outcomes.
Results: Despite the challenges of working with a poor patient population in a developing country, researchers were able to schedule follow-up appointments and obtain complete pre-operative and post-operative data sets on 70 patients for analysis; only 13 patients were lost to follow-up. Patients showed statistically significant improvements in the physical component summary, physical functioning, role-physical functioning and mental health sections of their SF-12v2 scores as well as their Quick DASH scores at 6 months post-operatively. No significant correlations were found with these surgical outcome measures and socioeconomic status evaluated through PPI and ELCSA scores.
Conclusions: Honduran patients with upper extremity problems that received surgical repairs as part of this short-term surgical mission have decreased upper extremity morbidity and improved health-related quality of life 6 months post-operatively. Notably, changes in patient SF-12v2 and Quick DASH scores 6 months post-operatively were not significantly correlated with measures of patient socioeconomic status, indicating that surgical missions targeting even the poorest of patients can be successful.
Furthermore, this study shows that follow-up studies of patients of short-term medical missions in developing countries are becoming increasingly feasible with the spread of mobile phones, allowing for post-mission follow-up months later with even the most difficult to access of patients. Overall, the results of this study indicate that this short-term mission had a significant positive impact on its surgical patients that could be quantitatively measured using research-validated survey tools. This study provides a model for other short-term medical missions to quantitatively measure their impact, so that in the future comparative analysis and determination of best practices in short-term medical missions might be possible.
Related articles