Abstract
Purpose: To elicit information about documentation and management of osteoporosis during inpatient episode among patients presenting for hip fracture fixation in a single surgeon’s high volume traumatology practice.
Introduction: Osteoporosis and osteopenia are common conditions characterized by decreased bone mass and increased fracture risk in postmenopausal women and both elderly males and females. Treatment for osteoporosis in patients older than 50 years is often not initiated because of the asymptomatic and slowly progressive nature of the disease.1 Many patients will not be evaluated and/or treated until it is recognized in conjunction with a fragility fracture.2 The initiation of osteoporosis treatment following hip fractures occurs at the low rates estimated at between 5% and 30%.3 A history of hip fractures is predictive of a 5% risk of another hip fracture within a year, a 17 to 21% risk of any fracture within 16 to 21 months, and a 29% risk of another hip fracture in the following 20 years.4 According to the literature, it is not standard practice among orthopaedic surgeons to manage osteoporosis after a hip fracture and subsequent surgery; however, recent studies have demonstrated that active participation of orthopaedic surgeons in the management of osteoporosis after a hip fracture greatly improves treatment rates.3,5 Eisman et al. proposed the Fracture Liaison Services , a secondary prevention program designed to incidence of future fractures in osteoporosis patients by utilizing a coordinator for risk assessment and linkage to the acute care provider, most often the orthopaedic surgeon, with the patients’ long-term or primary care provider for maintenance of ongoing osteoporosis management.6 Lugan et al. investigated callus formation by evaluating callus size, radiodensity and symmetry.7 The current investigation will examine the relationship between serum calcium levels both pre- and post-operatively and callus formation. The investigators hypothesized that patients treated operatively for hip fracture would not be routinely identified as osteoporotic at admission nor recommended for treatment at discharge.
Methods: We performed chart reviews for patients with surgical HF treatment in a single surgeon’s practice from 6/11 to 7/12. Inclusion criteria: age ≥ 55 years, femoral neck or intertrochanteric HF, hemiarthroplasty, intramedullary nail or cannulated screw fixation. Exclusions: high energy trauma, pathological fracture, nonoperative management. Measures/Outcomes:OP diagnosis/medication on admission, initiation of calcium & vitamin D during admission, OP documentation on discharge.
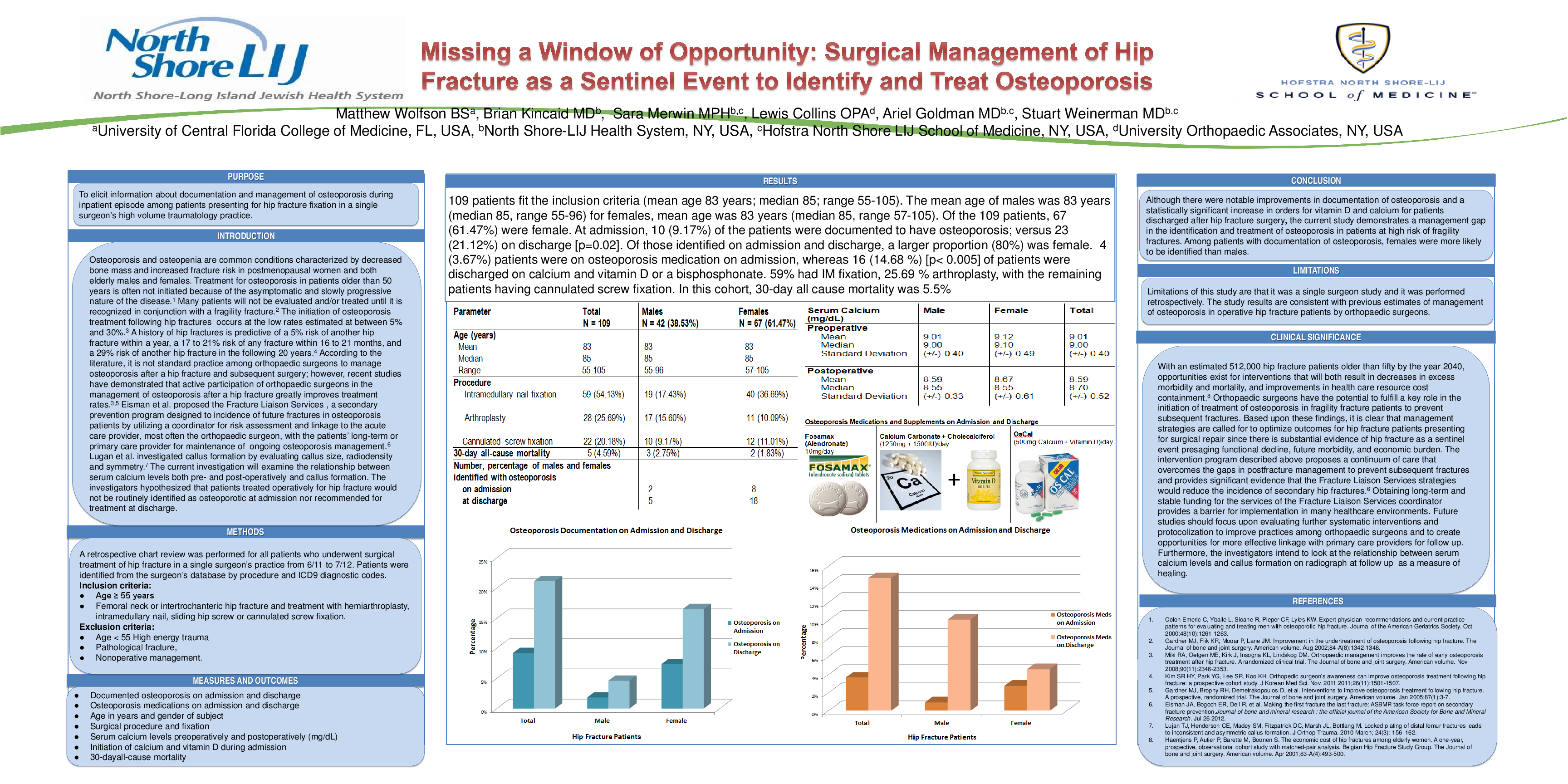
Results: 109 patients fit the inclusion criteria (mean age 83 years; median 85; range 55-105). The mean age of males was 83 years (median 85, range 55-96) for females, mean age was 83 years (median 85, range 57-105). Of the 109 patients, 67 (61.47%) were female. At admission, 10 (9.17%) of the patients were documented to have osteoporosis; versus 23 (21.12%) on discharge [p=0.02]. Of those identified on admission and discharge, a larger proportion (80%) was female. 4 (3.67%) patients were on osteoporosis medication on admission, whereas 16 (14.68 %) [p< 0.005] of patients were discharged on calcium and vitamin D or a bisphosphonate. 59% had IM fixation, 25.69 % arthroplasty, with the remaining patients having cannulated screw fixation. In this cohort, 30-day all cause mortality was 5.5%
Conclusions: Although there were notable improvements in documentation of OP & a statistically significant increase in calcium and vitamin D orders after discharge for HF surgery, the study demonstrates a management gap in the identification & treatment of OP in patients at high risk of fragility fractures for secondary prevention. Among patients with documentation of OP, females were more likely to be identified than males. Results are consistent with previous estimates of OP management in operative HF patients by OS. Based on these findings, management strategies are called for to optimize outcomes for HF patients presenting for surgical repair since there is substantial evidence of HF as a sentinel event presaging functional decline, future morbidity, and economic burden.Future studies should focus on systematic interventions to improve practices among OS & to create opportunities for more effective linkage with primary care providers for follow up.