Overwhelming Occlusion: A Case Of Extensive Arterial Thromboembolism Despite Treatment With Dabigatran
Abstract
Introduction: Dabigatran (Pradaxa) is a new direct thrombin inhibitor, indicated for cardioembolic protection from atrial fibrillation. In the RE-LY trial, dabigatran dosed at 150 mg twice daily was associated with lower rates of stroke and systemic embolism when compared to warfarin. There is, however, little information available concerning dabigatran’s ability to prevent thromboemboli in other disease states.
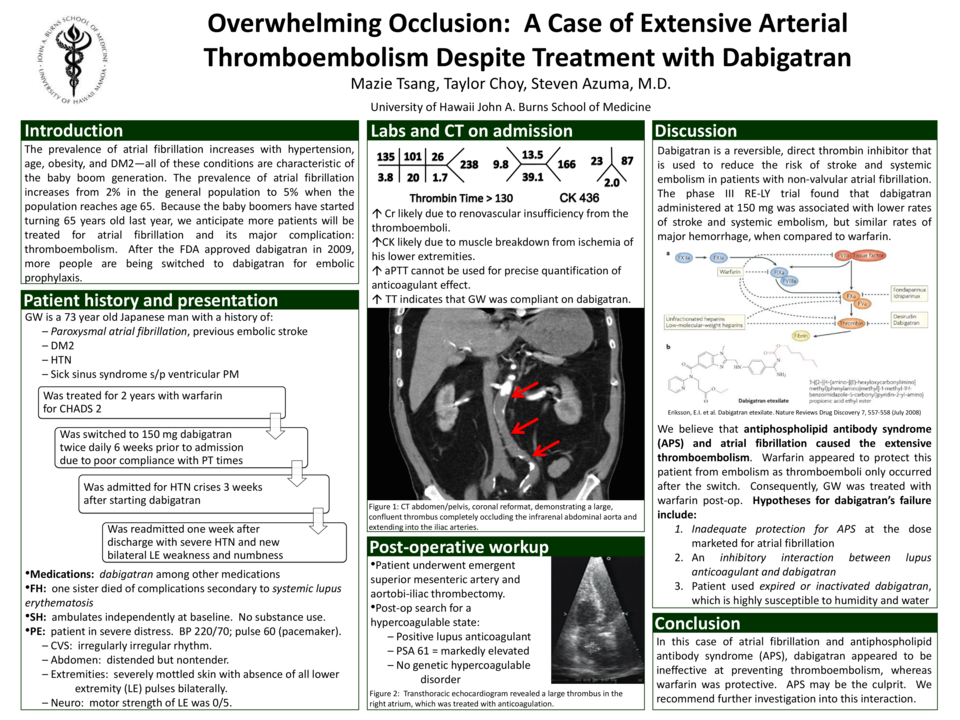
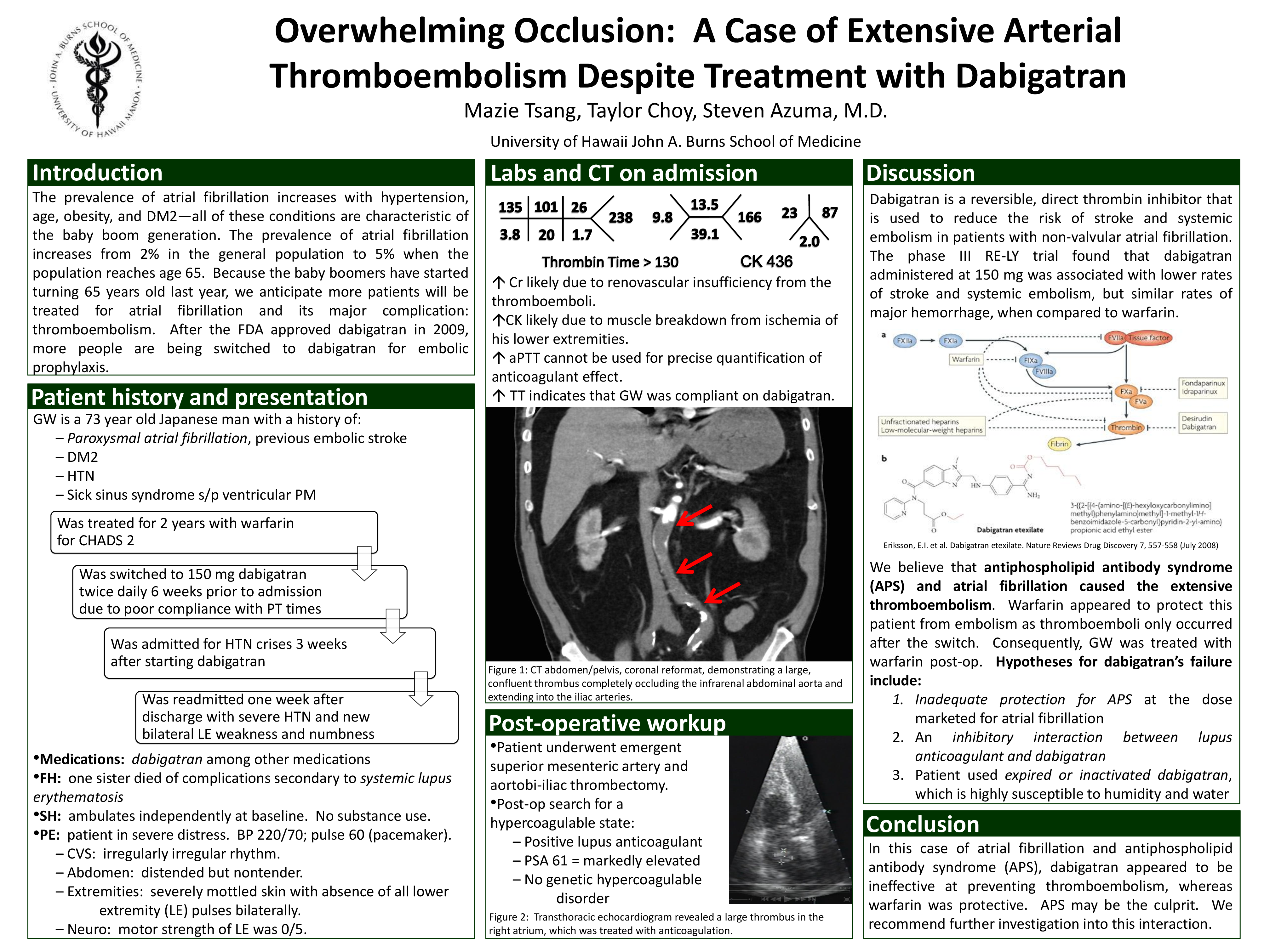
Case Report: A 73 year-old Asian man was brought to the hospital for sudden onset of bilateral lower extremity paralysis and back pain. He was previously diagnosed with paroxysmal atrial fibrillation two years prior to admission, which was treated with warfarin for a CHADS score of 4. Six weeks prior to admission, he was switched to dabigatran 150 mg twice daily. On admission, his blood pressure was 220/70. On physical exam, he was noted to have absent femoral and distal pulses bilaterally. Coagulation studies revealed an activated partial thromboplastin time (aPTT) of 87 and a thrombin time greater than 130. Contrast-enhanced CT of the chest/abdomen/pelvis revealed the following: a large thrombus occluding the distal infrarenal abdominal aorta with extension into the iliac arteries bilaterally; emboli to the superior mesenteric artery (SMA) and posterior branch of the left renal artery; bilateral renal infarcts; and a possible left atrial thrombus. The patient underwent thromboembolectomy of the SMA, aorta, and bilateral iliac arteries. He subsequently regained lower extremity pulses. Post-operative transthoracic echocardiogram suggested a large thrombus in the right atrium not present prior to admission. A workup for hypercoagulable disorders was significant for a PTT-lupus anticoagulant screen of 70 seconds confirmed with a positive hexagonal phase assay. The patient was bridged to warfarin with unfractionated heparin with no further embolic events.
Case discussion: This patient had no embolic events on warfarin, but after 6 weeks on dabigatran, he presented with thrombus in his right atrium and extensive arterial emboli. Atrial fibrillation is not associated with such a large degree of arterial emboli; this patient’s positive lupus anticoagulant suggests that antiphospholipid syndrome (APS) is the culprit. What makes this case unique is that outpatient treatment with dabigatran 150 mg twice daily did not prevent thromboemboli from atrial fibrillation with APS while warfarin appeared to be protective. We are uncertain why dabigatran failed to protect this patient with atrial fibrillation and APS from thromboemboli. Possible explanations include an inhibitory interaction between lupus anticoagulant and dabigatran.
Given the lack of clinical data regarding dabigatran and APS, physicians should be aware of possible interactions that render dabigatran ineffective. If a patient on dabigatran develops unexpected thromboembolism, one should consider pursuing an underlying hypercoagulable disorder, particularly APS. Further investigation into the apparent interaction between APS and dabigatran is recommended.
Related articles