Comparing Emergency Medicine Practices for Central Venous Catheter Placement to Existing ICU Checklists
Abstract
Background:
The incidence of Central Venous Catheter (CVC) insertion is increasing in the Emergency Department (ED). Checklists for CVC placement have been shown to increase adherence to best practices and reduce central line associated blood stream infections. Though multiple checklists have been published for use in the Intensive Care Unit (ICU), none has been tailored to the ED.
Objective:
Perform a pilot study to assess ED utilization of well accepted CVC checklists and determine adherence to specific checklist elements related to infection control.
Methods:
This was a convenience sample of CVC insertions in an urban Level I trauma ED performed between June and August 2011. CVC insertions by ED physicians were captured by an independent, trained observer on staggered shifts including days, evenings, and overnights. “Crash” CVC insertions (defined as placed under imminent life or death conditions) were excluded. Observed ED CVC placements were compared to elements of four non-ED checklists. We used descriptive statistics to identify areas of high and low adherence.
Results:
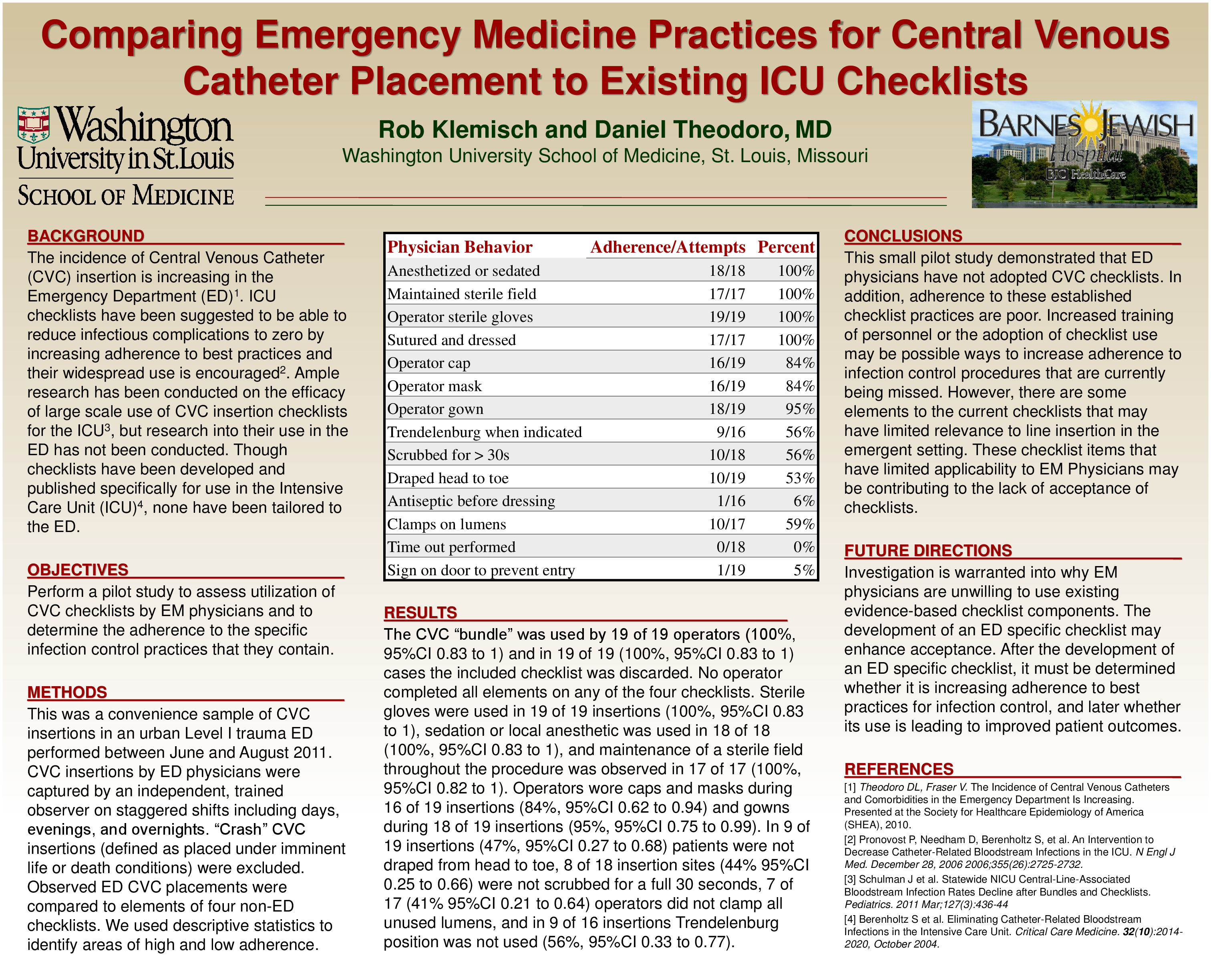
The CVC “bundle” was used by 19 of 19 operators (100%, 95%CI 0.83 to 1) and in 19 of 19 (100%, 95%CI 0.83 to 1) cases the included checklist was discarded. No operator completed all elements on any of the four checklists. Sterile gloves were used in 19 of 19 insertions (100%, 95%CI 0.83 to 1), sedation or local anesthetic was used in 18 of 18 (100%, 95%CI 0.83 to 1), and maintenance of a sterile field throughout the procedure was observed in 17 of 17 (100%, 95%CI 0.82 to 1). Operators wore caps and masks during 16 of 19 insertions (84%, 95%CI 0.62 to 0.94) and gowns during 18 of 19 insertions (95%, 95%CI 0.75 to 0.99). In 9 of 19 insertions (47%, 95%CI 0.27 to 0.68) patients were not draped from head to toe, 8 of 18 insertion sites (44% 95%CI 0.25 to 0.66) were not scrubbed for a full 30 seconds, 7 of 17 (41% 95%CI 0.21 to 0.64) operators did not clamp all unused lumens, and in 9 of 16 insertions Trendelenburg position was not used (56%, 95%CI 0.33 to 0.77).
Conclusions:
This small pilot study demonstrated that ED physicians have not adopted CVC checklists. In addition, adherence to these established checklist practices are poor. Outcomes of ED central lines may benefit from an ED developed, structured checklist.
Related articles