Association of Third Trimester Abdominal Circumference With Provider-initiated Preterm Delivery
Abstract
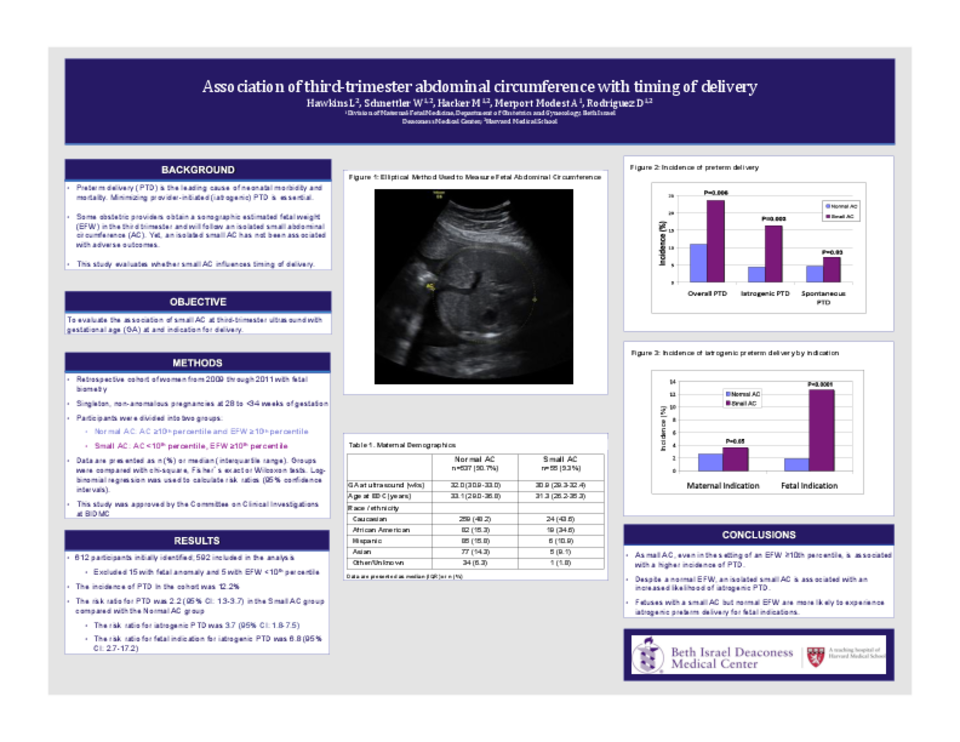
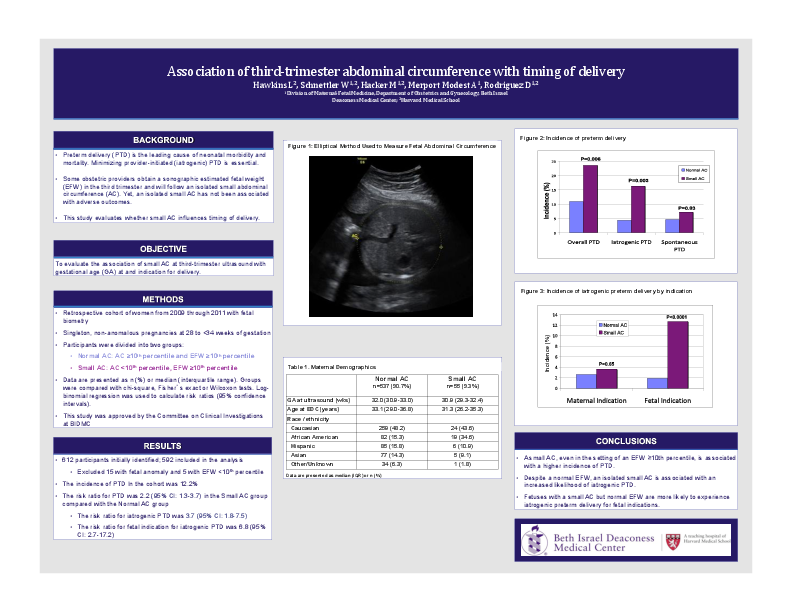
Objectives: To evaluate the association of small abdominal circumference (AC <10th percentile) at third trimester ultrasound with gestational age (GA) at delivery, indication for delivery and neonatal outcomes.
Methods: All women seen at our institution from 2010 through 2011 for measurements from 28 to 34 weeks’ gestation with a singleton, non-anomalous pregnancy were included in this retrospective cohort. Three groups were defined based on biometric results from each woman’s single earliest ultrasound in this window: “Normal” fetuses with normal AC and normal estimated fetal weight (EFW; both ≥10th percentile), “Small AC” fetuses with AC < 10th percentile and normal EFW, and “IUGR” fetuses with AC and EFW < 10th percentile. Comparisons were made between groups for GA at delivery, indication for delivery, and neonatal outcomes. Indications for delivery were categorized as either provider-initiated or spontaneous by review of the operative/delivery reports in the medical record. Data are presented as medians, interquartile ranges (IQR) and risk ratios (RR) with 95% confidence intervals (CI).
Results: 597 women met eligibility criteria, and demographic data was similar throughout the cohort. The median GA at ultrasound was 32.0 weeks (IQR: 30.6-33.0) and median maternal age at delivery was 32.9 years (IQR: 28.8-36.7). A small AC was found in 10.6% of the fetuses. The incidence of pre-term delivery (PTD) in the cohort was 12.2%.
Compared to Normal fetuses, those in the Small AC group had a higher incidence of preterm delivery. Small AC fetuses were more than twice as likely to be delivered preterm than Normal fetuses [RR= 2.2; 95% CI (1.3-3.7)], more than three times as likely to experience provider-initiated PTD [RR=3.7; 95% CI (1.8-7.5)] and more than six times as likely to experience provider-initiated PTD for a fetal indication [RR=6.8; 95% CI (2.7-17.2)]. Two-thirds of the provider-initiated preterm deliveries in the Small AC group included concerns for fetal growth in the indication compared to only 8.3% in the Normal group (p<0.01). Of the 5 fetuses in the IUGR group, all were provider-initiated preterm deliveries with concern for fetal growth included in the indication. The RRs did not change appreciably after adjusting for maternal age and race/ethnicity. No significant differences in immediate neonatal outcomes between the Normal and Small AC group were witnessed aside from an expected difference in mean birth weight.
Conclusions: Small AC, even in the setting of an EFW ≥10th percentile, is associated with a higher incidence of PTD; specifically provider-initiated preterm delivery. Fetal growth concerns and other fetal indications appeared to drive the decision for these fetuses’ deliveries. Immediate neonatal outcomes were similar to the Normal group challenging the need for provider-initiated preterm delivery of fetuses with isolated small AC. Further investigation into the rationale for preterm delivery and long-term neonatal outcomes of such fetuses is warranted.
Related articles