Primary Radiotherapy versus Radical Prostatectomy for High-risk Prostate Cancer: A Decision Analysis
Abstract
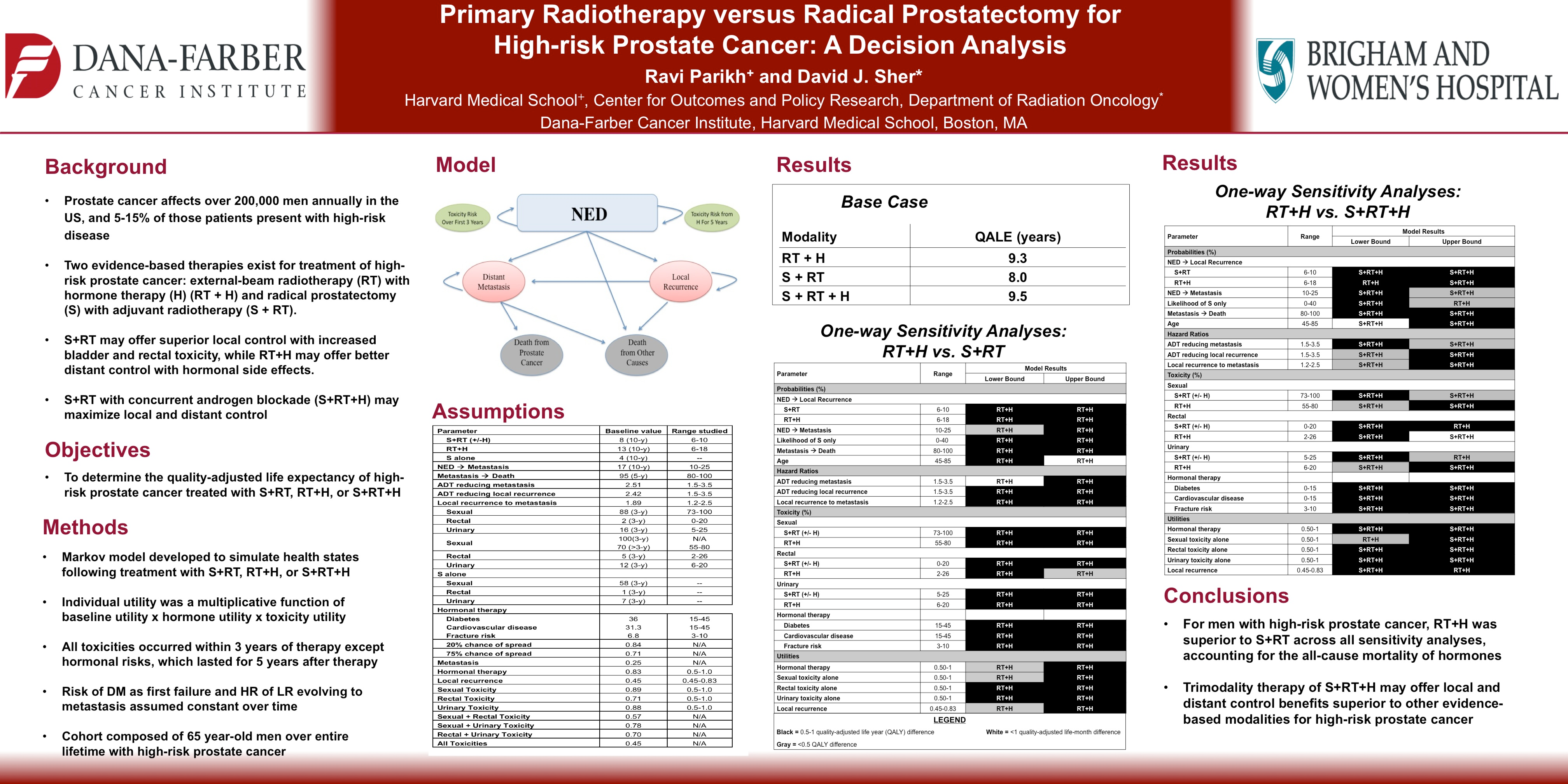
Purpose: Prostate cancer is diagnosed in over 200,000 men annually in the United States, with up to 25% presenting with high-risk disease. Two evidence-based therapies exist for the treatment of high-risk prostate cancer: external beam radiation therapy with androgen deprivation therapy (RT+H) and radical prostatectomy with adjuvant radiation therapy (S+RT). These strategies have never been compared in a prospective trial. Using decision analysis, we compared the quality-adjusted life expectancy (QALE) among men treated for high-risk prostate cancer with RT+H versus S+RT versus a hypothetical trimodality therapy consisting of S+RT with concurrent androgen blockade (S+RT+H).
Patients and Methods: We developed a Markov model to describe lifetime health states after treatment for high-risk prostate cancer. Probabilities and utilities were extrapolated from the literature: local control rates following S+RT were abstracted from SWOG 8794, and local control rates for RT+H were taken from RTOG 9202. All patients were assumed to have the same rate of distant metastasis (DM) before treatment. The relative efficacy of H in the S+RT+H arm was modeled from RTOG 9202 and 8610. Toxicity rates following RT were based on recent IMRT series, and patients were exposed to risks of diabetes, cardiovascular disease, and osteoporotic fracture for 5 years after completing H. Sensitivity analyses were carried out to model uncertainty in outcome rates, toxicities, and utilities.
Results: In the base case, the QALE following treatment with RT+H, S+RT, and S+RT+H were 9.3, 8.0, and 9.5 quality adjusted life years (QALYs), respectively. RT+H resulted in an increase of at least 1 QALY compared to S+RT in nearly all one-way sensitivity analyses. The difference between the two treatments was notably less than 1 QALY when assuming a low DM rate. In contrast, S+RT+H was in most cases superior to RT+H, but by small margins (< 0.5 QALY). Differences were highly sensitive to toxicity assumptions, and RT+H was associated with a 0-1 QALY benefit over S+RT+H in five scenarios, including a high risk of bowel toxicity after surgery and low utility of impotence.
Conclusion: In comparison to prostatectomy and adjuvant RT, radiotherapy with androgen deprivation was the optimal treatment strategy for treatment of high-risk prostate cancer. Furthermore, despite increased morbidity compared to evidence-based strategies, trimodality therapy is associated with local and distant control benefits that may lead to superior outcomes in a meaningful population of men. The sensitivity of this comparison to toxicity assumptions suggests that patient preference of potential outcomes must govern use of trimodality therapy. Such a strategy warrants further study.
Related articles