The Role of Margin Status and Radiation Dose in Determining Local Recurrence Rate After Breast-Conserving Therapy
Abstract
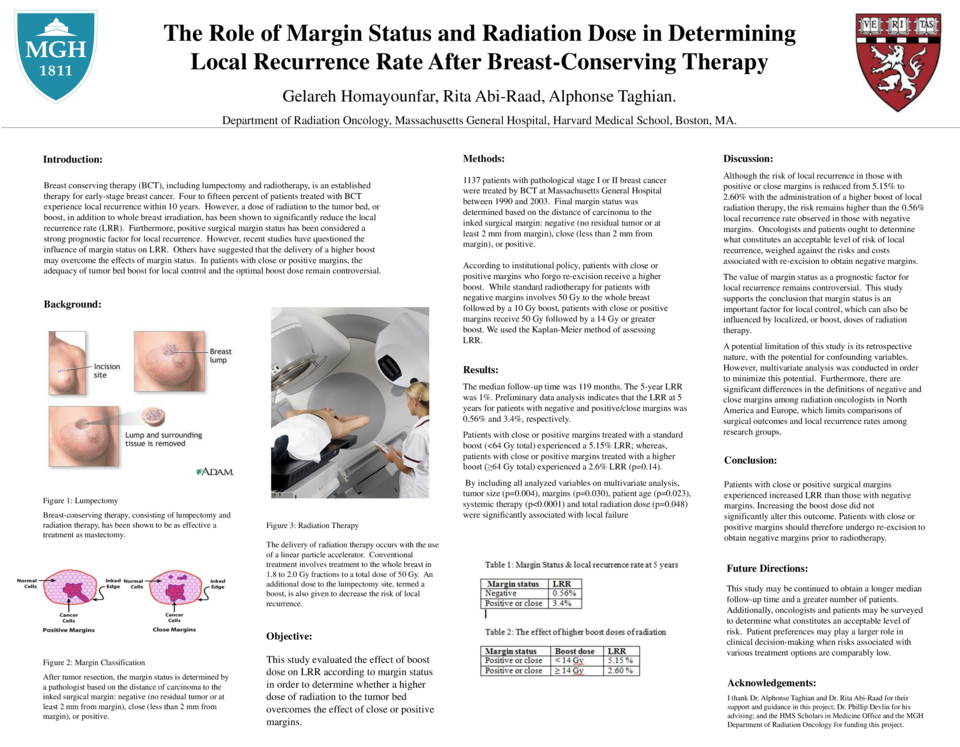
Objective: Breast conserving therapy (BCT), including lumpectomy and
radiotherapy, is an established therapy for early-stage breast cancer. Four to fifteen
percent of patients treated with BCT experience local recurrence within 10 years.
However, a dose of radiation to the tumor bed, or boost, in addition to whole breast
irradiation, has been shown to significantly reduce the local recurrence rate (LRR).
Furthermore, positive surgical margin status has been considered a strong prognostic
factor for local recurrence. However, recent studies have questioned the influence of
margin status on LRR. Others have suggested that the delivery of a higher boost may
overcome the effects of margin status. In patients with close or positive margins, the
adequacy of tumor bed boost for local control and the optimal boost dose remain
controversial. This study evaluated the effect of boost dose on LRR according to margin
status in order to determine whether a higher dose of radiation to the tumor bed
overcomes the effect of close or positive margins.
Materials/Methods: 1137 patients with pathological stage I or II breast cancer were treated by BCT at Massachusetts General Hospital between 1990 and 2003. Final margin status was determined based on the distance of carcinoma to the inked surgical margin: negative (no residual tumor or at least 2 mm from margin), close (less than 2 mm from margin), or positive. According to institutional policy, patients with close or positive margins who forgo re-excision receive a higher boost. While standard radiotherapy for patients with negative margins involves 50 Gy to the whole breast followed by a 10 Gy boost, patients with close or positive margins receive 50 Gy followed by a 14 Gy or greater boost. We used the Kaplan-Meier method of assessing LRR.
Results: The median follow-up time was 119 months. The 5-year LRR was 1%. Preliminary data analysis indicates that the LRR at 5 years for patients with negative and positive/close margins was 0.56% and 3.4%, respectively. Patients with close or positive margins treated with a standard boost (<64 Gy total) experienced a 5.15% LRR; whereas, patients with close or positive margins treated with a higher boost (≥64 Gy total) experienced a 2.6% LRR (p=0.14). By including all analyzed variables on multivariate analysis, tumor size (p=0.004), margins (p=0.030), patient age (p=0.023), systemic therapy (p<0.0001) and total radiation dose (p=0.048) were significantly associated with local failure.
Conclusions: Patients with close or positive surgical margins experienced
increased LRR than those with negative margins. Increasing the boost dose did not
significantly alter this outcome. Patients with close or positive margins should therefore
undergo re-excision to obtain negative margins prior to radiotherapy.
Related articles