Abstract
Background: Uninsured individuals experience lower breast cancer screening rates and higher breast cancer morbidity and mortality than insured populations. In Arizona, the 2020 breast cancer screening rate was 42% among uninsured individuals compared with 63% statewide. The Well Woman HealthCheck Program (WWHP) offers free breast cancer screening regardless of documentation status; however, national utilization remains low. Within the University of Arizona Commitment to Underserved People (CUP) student-run free clinics, the baseline breast cancer screening rate was 21.7%.
Objective: To increase breast cancer screening among uninsured patients assigned female at birth aged 40–64 years receiving care at CUP clinics by 13.3%, achieving the national uninsured screening benchmark of 35% within 12 months.
Methods: A quality improvement initiative was implemented from September 2023 through August 2024 using the Institute for Healthcare Improvement Model for Improvement framework. A referral workflow was developed to connect eligible patients to the WWHP. Four Plan-Do-Study-Act cycles were completed to refine implementation. The primary outcome measure was the proportion of eligible patients completing mammography during the study period. The process measure was completion of a bilingual screening questionnaire administered to eligible patients.
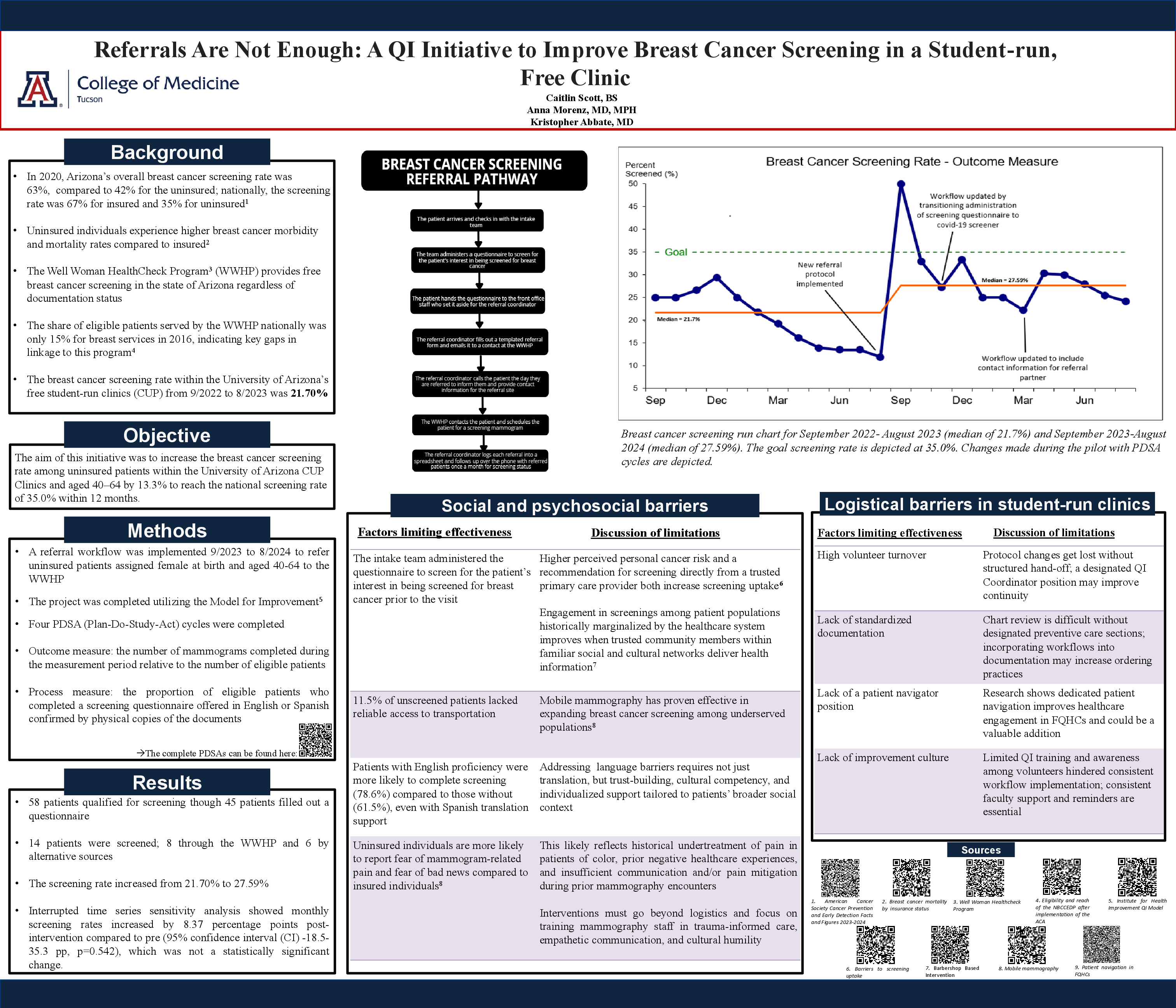
Results: Fifty-eight patients met screening criteria, and 45 completed the questionnaire. Fourteen patients completed screening mammography, including 8 through the WWHP and 6 through alternative sources. The clinic screening rate increased from 21.7% pre-intervention to 27.6% post-intervention. Interrupted time series sensitivity analysis demonstrated a post-intervention monthly increase of 8.37 percentage points compared with baseline; however, this did not reach statistical significance (95% CI, -18.5 to 35.3; p=0.542).
Conclusions: A referral-based workflow modestly improved breast cancer screening rates in a student-run free clinic but did not achieve the target benchmark. Persistent barriers included transportation, language discordance, fear of screening, volunteer turnover, limited documentation systems, and absence of patient navigation. Future efforts should incorporate patient navigators, culturally responsive outreach, improved continuity processes, and mobile screening access to enhance preventive care uptake in underserved populations.