Abstract
Accounting for up to 20 percent of pediatric emergency department visits annually, fever contributes substantially to healthcare utilization. Fever of unknown origin, or a fever with extended duration, is less common and often results in clinical conundrums.
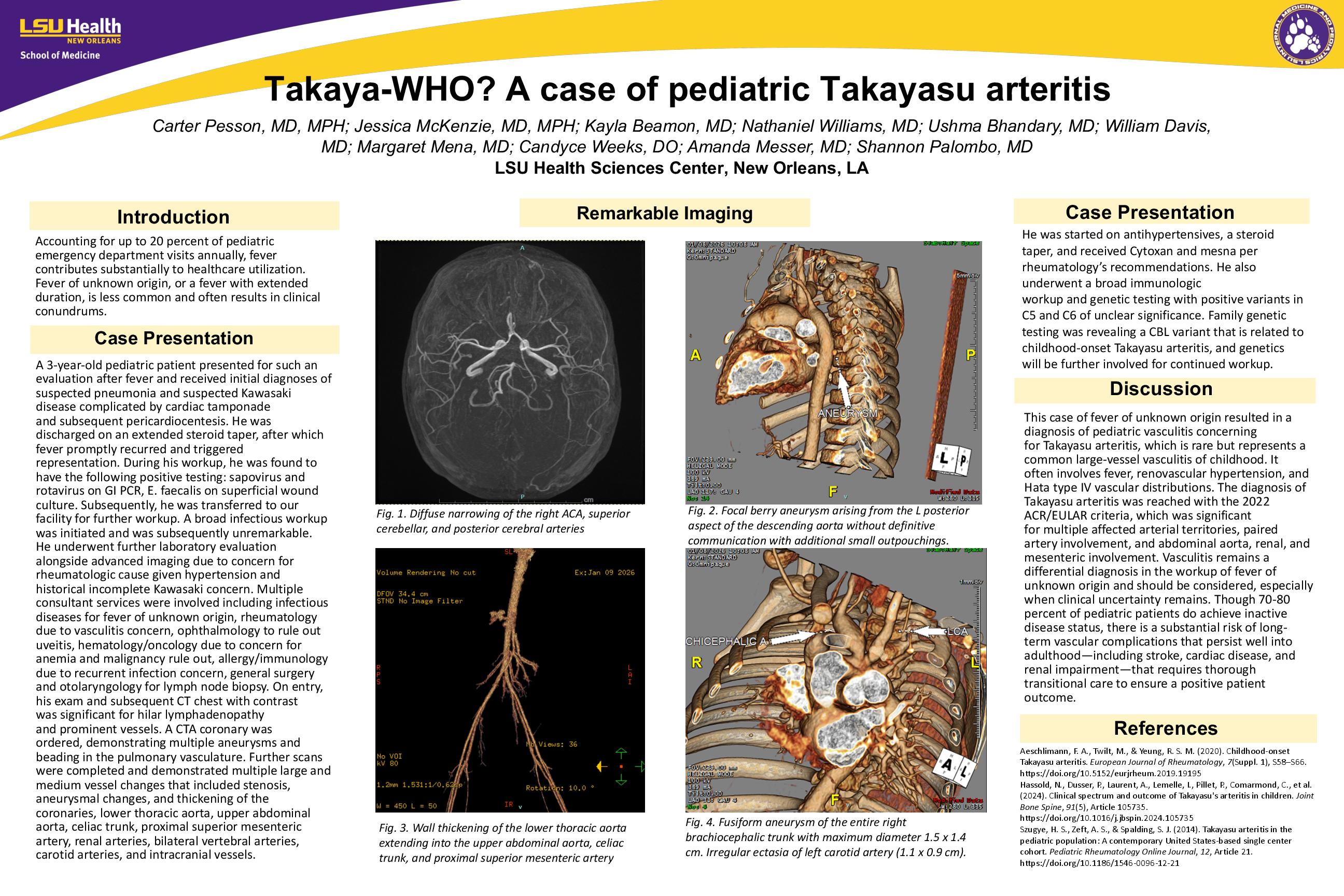
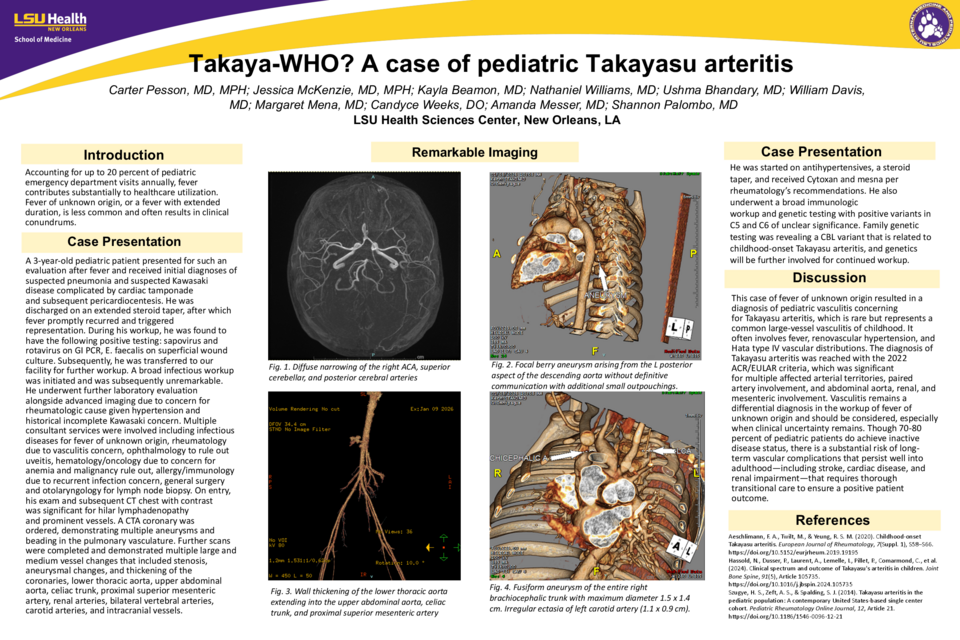
A 3-year-old pediatric patient presented for such an evaluation after fever and received initial diagnoses of suspected pneumonia and suspected Kawasaki disease complicated by cardiac tamponade and subsequent pericardiocentesis. He was discharged on an extended steroid taper, after which fever promptly recurred and triggered representation. During his workup, he was found to have the following positive testing: sapovirus and rotavirus on GI PCR, E. faecalis on superficial wound culture. Subsequently, he was transferred to our facility for further workup. A broad infectious workup was initiated and was subsequently unremarkable. He underwent further laboratory evaluation alongside advanced imaging due to concern for rheumatologic cause given hypertension and historical incomplete Kawasaki concern. Multiple consultant services were involved including infectious diseases for fever of unknown origin, rheumatology due to vasculitis concern, ophthalmology to rule out uveitis, hematology/oncology due to concern for anemia and malignancy rule out, allergy/immunology due to recurrent infection concern, general surgery and otolaryngology for lymph node biopsy. On entry, his exam and subsequent CT chest with contrast was significant for hilar lymphadenopathy and prominent vessels. A CTA coronary was ordered, demonstrating multiple aneurysms and beading in the pulmonary vasculature. Further scans were completed and demonstrated multiple large and medium vessel changes that included stenosis, aneurysmal changes, and thickening of the coronaries, lower thoracic aorta, upper abdominal aorta, celiac trunk, proximal superior mesenteric artery, renal arteries, bilateral vertebral arteries, carotid arteries, and intracranial vessels.
He was started on antihypertensives, a steroid taper, and received Cytoxan and mesna per rheumatology's recommendations. He also underwent a broad immunologic workup and genetic testing with positive variants in C5 and C6 of unclear significance. Family genetic testing was revealing a CBL variant that is related to childhood-onset Takayasu arteritis, and genetics will be further involved for continued workup.
This case of fever of unknown origin resulted in a diagnosis of pediatric vasculitis concerning for Takayasu arteritis, which is rare but represents a common large-vessel vasculitis of childhood. It often involves fever, renovascular hypertension, and Hata type IV vascular distributions. The diagnosis of Takayasu arteritis was reached with the 2022 ACR/EULAR criteria, which was significant for multiple affected arterial territories, paired artery involvement, and abdominal aorta, renal, and mesenteric involvement. Vasculitis remains a differential diagnosis in the workup of fever of unknown origin and should be considered, especially when clinical uncertainty remains. Though 70-80 percent of pediatric patients do achieve inactive disease status, there is a substantial risk of long-term vascular complications that persist well into adulthood—including stroke, cardiac disease, and renal impairment—that requires thorough transitional care to ensure a positive patient outcome.