Abstract
Background: Left ventricular non-compaction cardiomyopathy (LVNC) is an uncommon form of cardiomyopathy characterized by prominent myocardial trabeculations and deep intertrabecular recesses due to incomplete compaction of the ventricular myocardium during embryologic development. Patients with LVNC may develop progressive systolic heart failure, arrhythmias, and thromboembolic complications. Mechanical circulatory support with a left ventricular assist device (LVAD) is an established therapy for patients with advanced heart failure who are not candidates for cardiac transplantation. However, LVAD implantation in patients with LVNC can present technical challenges due to abnormal ventricular morphology and the potential for inflow cannula obstruction. Additionally, preoperative right ventricular dysfunction is associated with a higher risk of postoperative right heart failure following LVAD placement.
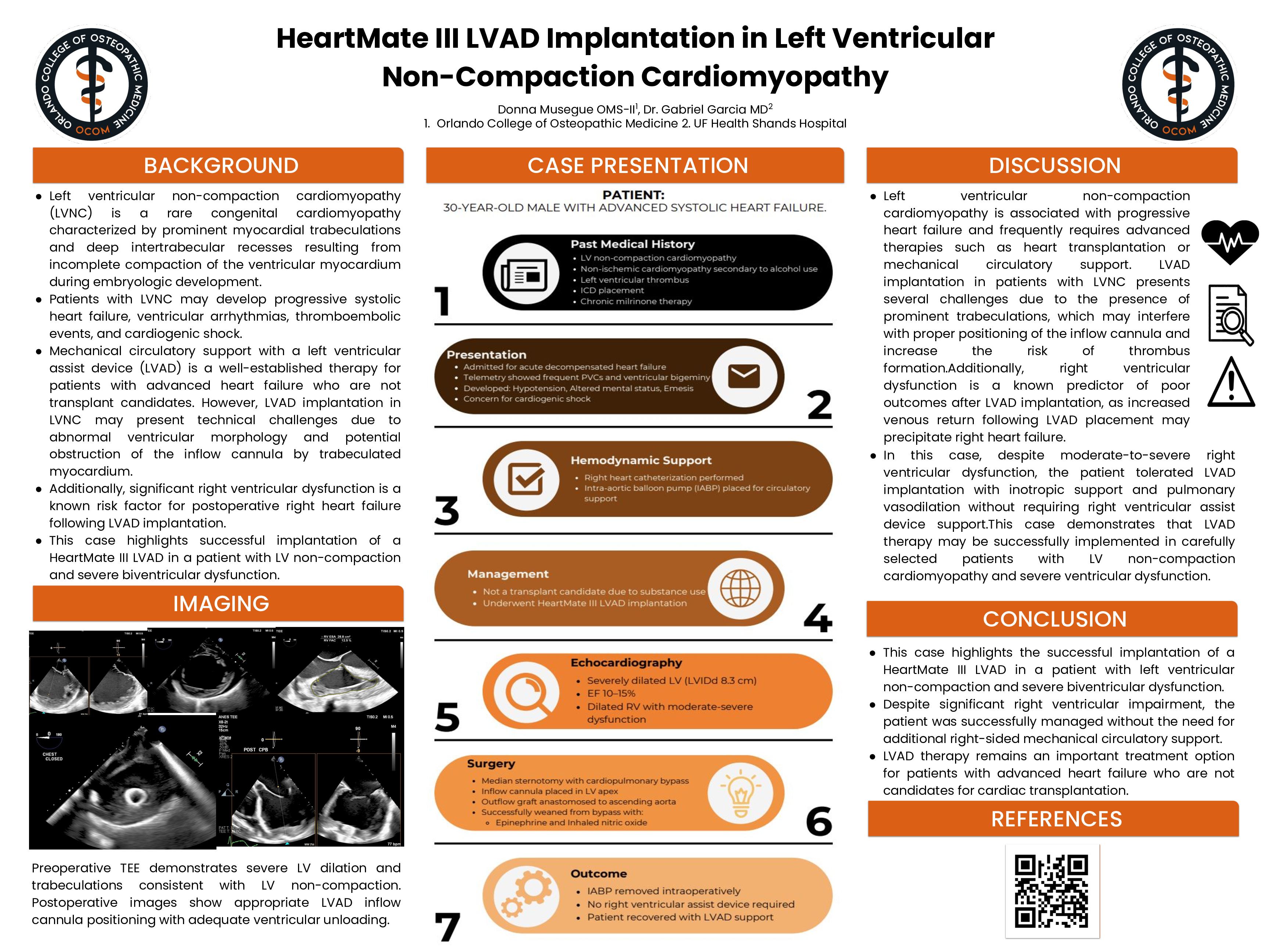
Case Presentation: We describe a 30-year-old male with chronic systolic heart failure secondary to non-ischemic cardiomyopathy related to alcohol use and known LVNC who was maintained on home milrinone therapy. The patient presented with acute decompensated heart failure and subsequently developed cardiogenic shock, with hypotension, altered mental status, and frequent ventricular ectopy on telemetry. Echocardiography demonstrated a severely dilated left ventricle (LVIDd 8.3 cm) with severely reduced systolic function (ejection fraction 10–15%) as well as moderate-to-severe right ventricular dysfunction. An intra-aortic balloon pump was placed for temporary hemodynamic support. Because the patient was not a candidate for heart transplantation due to ongoing substance use, he underwent implantation of a HeartMate III LVAD via median sternotomy. The inflow cannula was positioned in the left ventricular apex and the outflow graft was anastomosed to the ascending aorta. The patient was successfully weaned from cardiopulmonary bypass with inotropic support and inhaled nitric oxide. Despite significant preoperative right ventricular dysfunction, additional right-sided mechanical circulatory support was not required.
Discussion:LVAD implantation in patients with LVNC may be technically challenging due to the presence of prominent trabeculations that can interfere with inflow cannula positioning. In addition, right ventricular dysfunction is a known predictor of postoperative right heart failure after LVAD placement. In this case, careful surgical technique and perioperative hemodynamic management allowed successful LVAD implantation without the need for right ventricular assist device support.
Conclusion: This case demonstrates that HeartMate III LVAD implantation can be successfully performed in selected patients with left ventricular non-compaction cardiomyopathy and advanced heart failure. With appropriate perioperative management, LVAD therapy may provide an effective treatment option for patients who are not candidates for cardiac transplantation.