Abstract
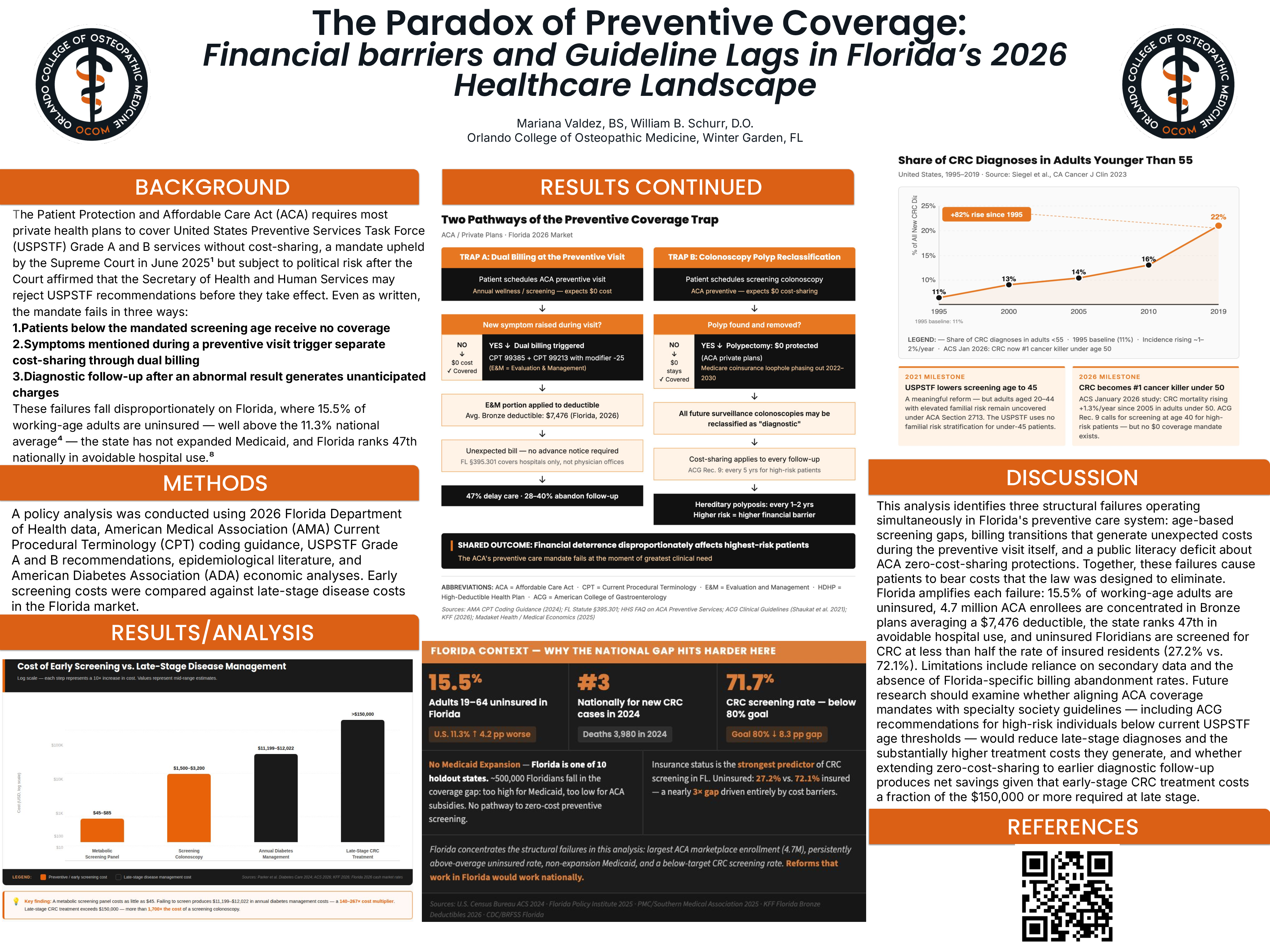
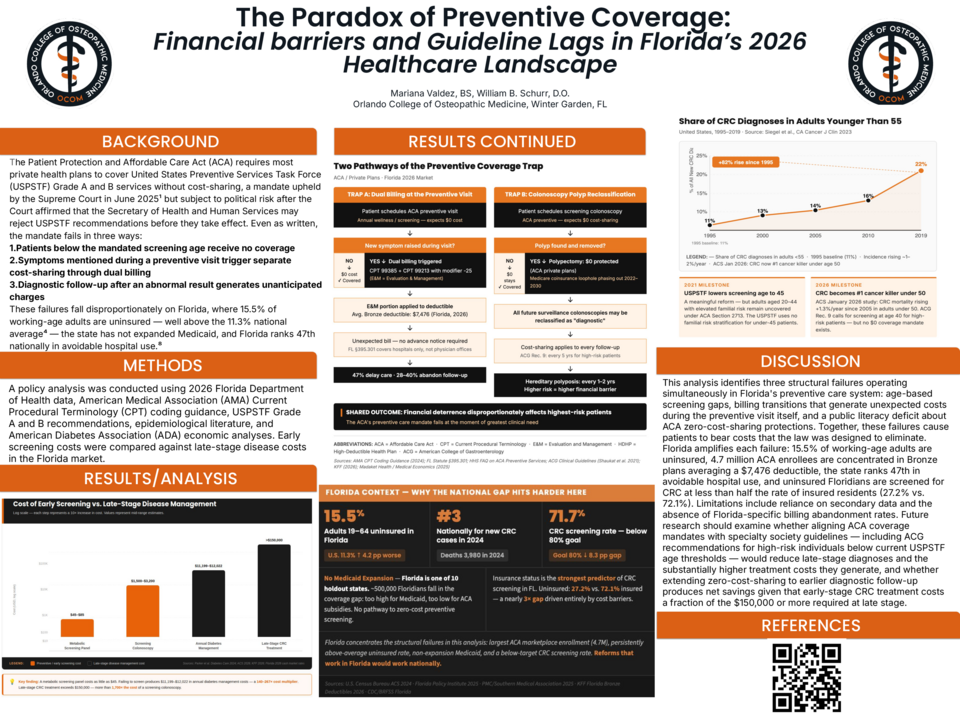
BACKGROUND Section 2713 of the ACA mandates coverage of USPSTF Grade A and B services without cost-sharing — upheld June 2025, though the ruling granted the HHS Secretary authority to reject Task Force recommendations. Three gaps persist: adults below screening age are excluded from zero-cost care, problems during a preventive visit trigger dual billing, and diagnostic follow-up is reclassified as non-preventive. These failures concentrate in Florida, where 15.5% of working-age adults are uninsured, Medicaid is not expanded, and the state ranks 47th in avoidable hospital use.
METHODS Policy analysis using Florida DOH data, AMA CPT guidelines, USPSTF and ACG recommendations, and peer-reviewed literature. Osteopathic Significance: Billing that fragments the preventive encounter contradicts the principle that structure and function are interrelated.
RESULTS Three failures were identified. First, USPSTF lowered CRC screening from 50 to 45 in 2021; adults 20–44 remain unprotected. Early-onset CRC rises 1–2% annually and is the leading cause of cancer death under 50. Florida ranked 3rd nationally in 2024 (11,920 cases; 3,980 deaths), rate 71.7% vs. 80% target. ACG Rec. 9 advises colonoscopy at 40 for high-risk patients — no ACA protection applies. Second, dual billing (CPT 99385 + 99213, modifier -25) applies the E&M charge to the deductible — $7,476 average on Florida Bronze plans. 47% of patients delayed care due to cost uncertainty; 28–40% of HDHP enrollees abandon follow-up after an unexpected bill. Third, metabolic panel: $45–$85 vs. $11,199–$12,022/year for type 2 diabetes and $150,000+ for late-stage CRC. Florida: 2.07M diagnosed diabetes, 5.97M prediabetes, $27.2B annual costs. CRC screening: 27.2% uninsured vs. 72.1% insured. SB 158 (January 2026) eliminated cost-sharing for breast imaging after an inconclusive mammogram — no equivalent exists for metabolic or gastrointestinal follow-up.
DISCUSSION Age-based exclusions, billing transitions that shift costs at the point of care, and limited understanding of coverage limits converge on the same population at the same clinical moment. Current ACA mandates trail specialty society standards — ACG Recommendation 9 identifies a high-risk population for whom earlier colonoscopy is clinically indicated, yet no zero-cost-sharing protection exists. Aligning coverage policy with specialty guidelines is a low-disruption, evidence-based path to closing the age gap without awaiting USPSTF updates. Three reforms are warranted: an expedited USPSTF interim at-risk Grade B pathway for high-risk adults below current thresholds; extension of SB 158 to metabolic and gastrointestinal follow-up; and mandatory written financial disclosure before any preventive visit at which additional cost-sharing may apply.