Abstract
Background:
Epiglottitis is a rare inflammatory condition characterized by edema of the epiglottis, aryepiglottic folds, arytenoids, and surrounding supraglottic tissues that can lead to life threatening airway obstruction. Historically, epiglottis was commonly caused by bacterial infection, specifically Haemophilus influenza type b. However, its incidence in children has significantly decreased since the introduction of vaccines. Epiglottitis presents with nonspecific symptoms including sore throat, dysphagia, muffled or “hot potato” voice, fever, and drooling.
Ludwig’s angina is a rare, life-threatening condition that presents with rapidly progressing cellulitis involving the soft tissues of the floor of the mouth and neck which can lead to airway obstruction. It often involves the three compartments of the floor of the mouth which include the sublingual, submental and submandibular spaces also known as the submandibular triangle. Ludwig’s angina is commonly due to odontogenic infections, and it presents similarly to adult epiglottitis such as diffuse neck swelling, dysphagia, and respiratory distress.
Both Ludwig’s angina and epiglottitis are uncommon in adults within the United States due to improved oral hygiene and vaccinations, respectively. However, both pathologies require immediate attention due to the possibility of life threatening airway compromise making prompt recognition and differentiation essential.
Case Presentation:
A 57-year-old female with a past medical history of cerebrovascular accident and hypertension presented to the emergency department with acute throat swelling that began a few hours earlier. She reported persistent throat swelling, nausea, vomiting, and a sensation of phlegm in the back of her throat despite self administration of Benadryl. She denied shortness of breath or chest pain.
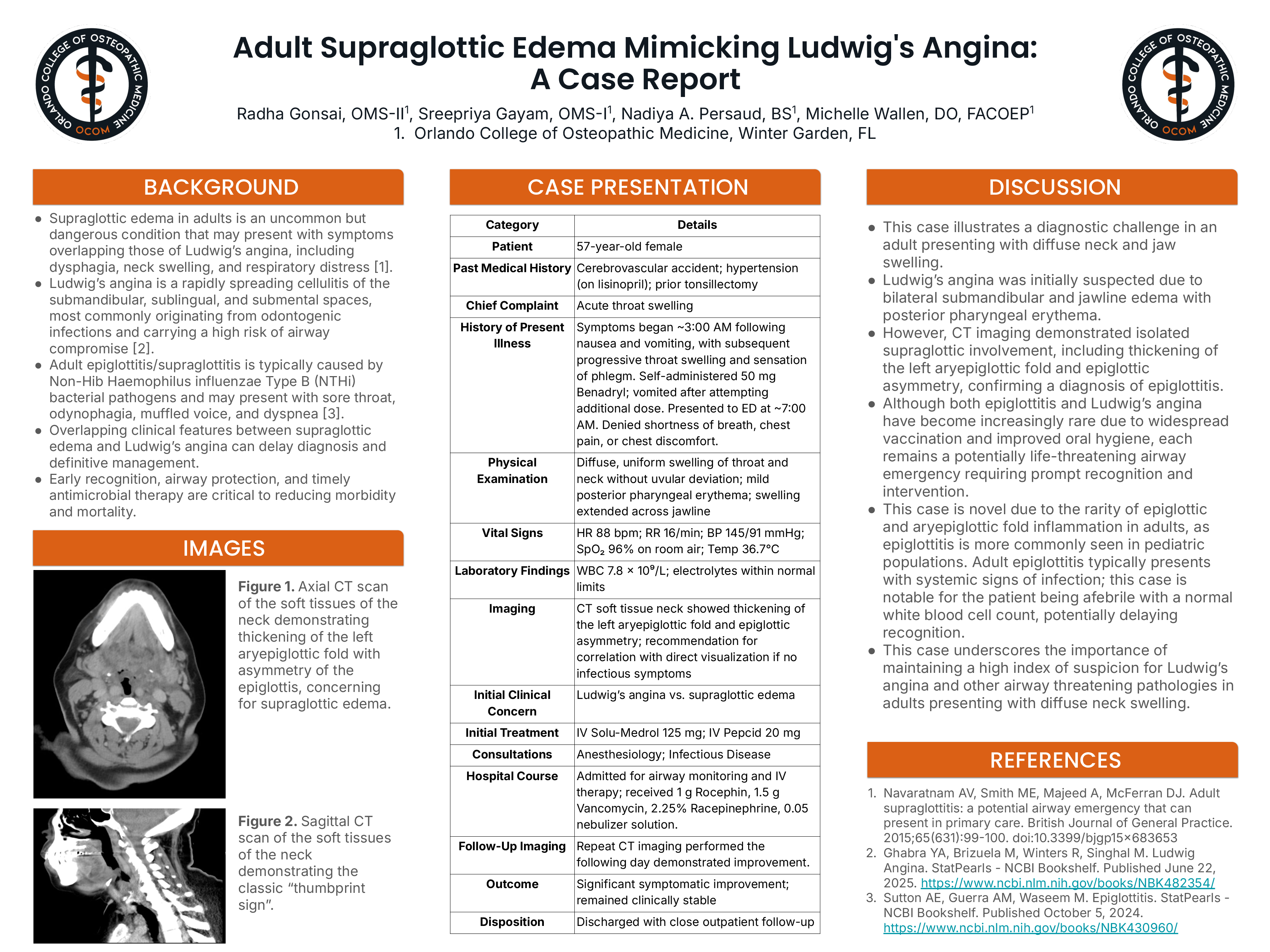
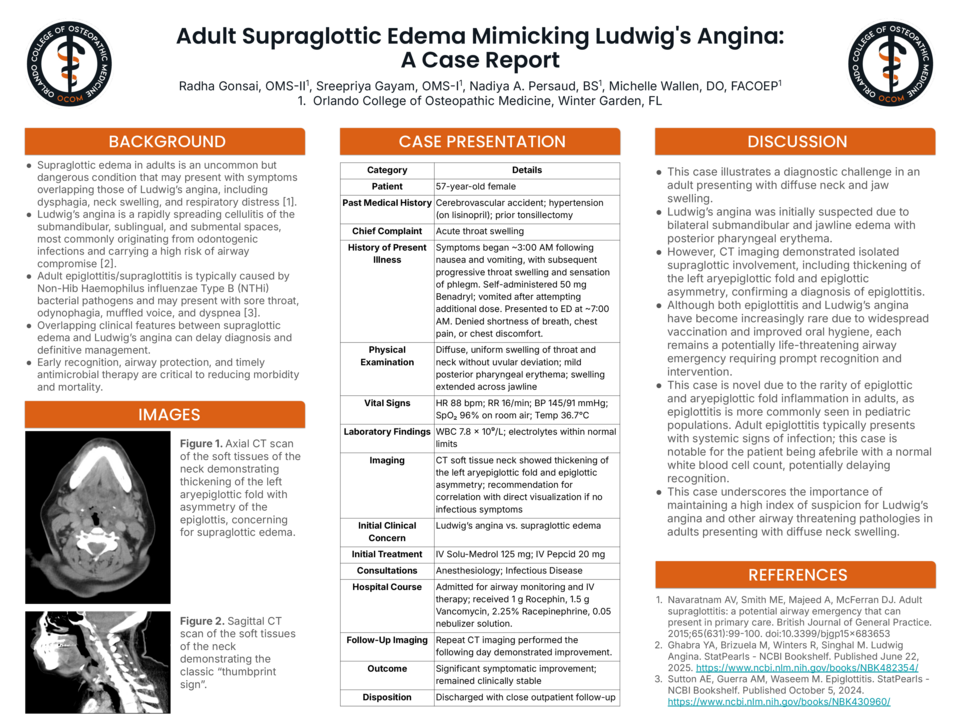
On examination, there was diffuse, uniform swelling of the throat and neck without uvular deviation. Mild irritation and erythema were noted at the back of the throat, with swelling extending to the neck and across the jawline. Her vital signs were stable. A CT scan with contrast of the soft tissue neck showed thickening of the left aryepiglottic fold and asymmetry of the epiglottis. The patient was treated with IV corticosteroids, IV antibiotics, and bronchodilators. A repeat CT was done the next day which showed improvement.
Discussion:
Given initial presentation of diffuse uniform neck swelling and subacute symptoms, the primary suspicion was Ludwig’s angina. However, CT imaging ultimately confirmed a diagnosis of epiglottitis. Additionally, the patient was afebrile with a normal white blood cell count and no signs of immediate airway compromise. This case is notable for the rarity of epiglottitis in adult populations and underscores the importance of maintaining a high index of suspicion for Ludwig’s angina and other potentially airway-compromising conditions in adults presenting with diffuse neck swelling.