Abstract
BACKGROUND
Myocardial infarction with non-obstructive coronary arteries (MINOCA) and Takotsubo syndrome (TTS) are two ST-elevation myocardial infarction (STEMI) mimics, and although they usually have defining features, they can present very similarly.
CASE PRESENTATION
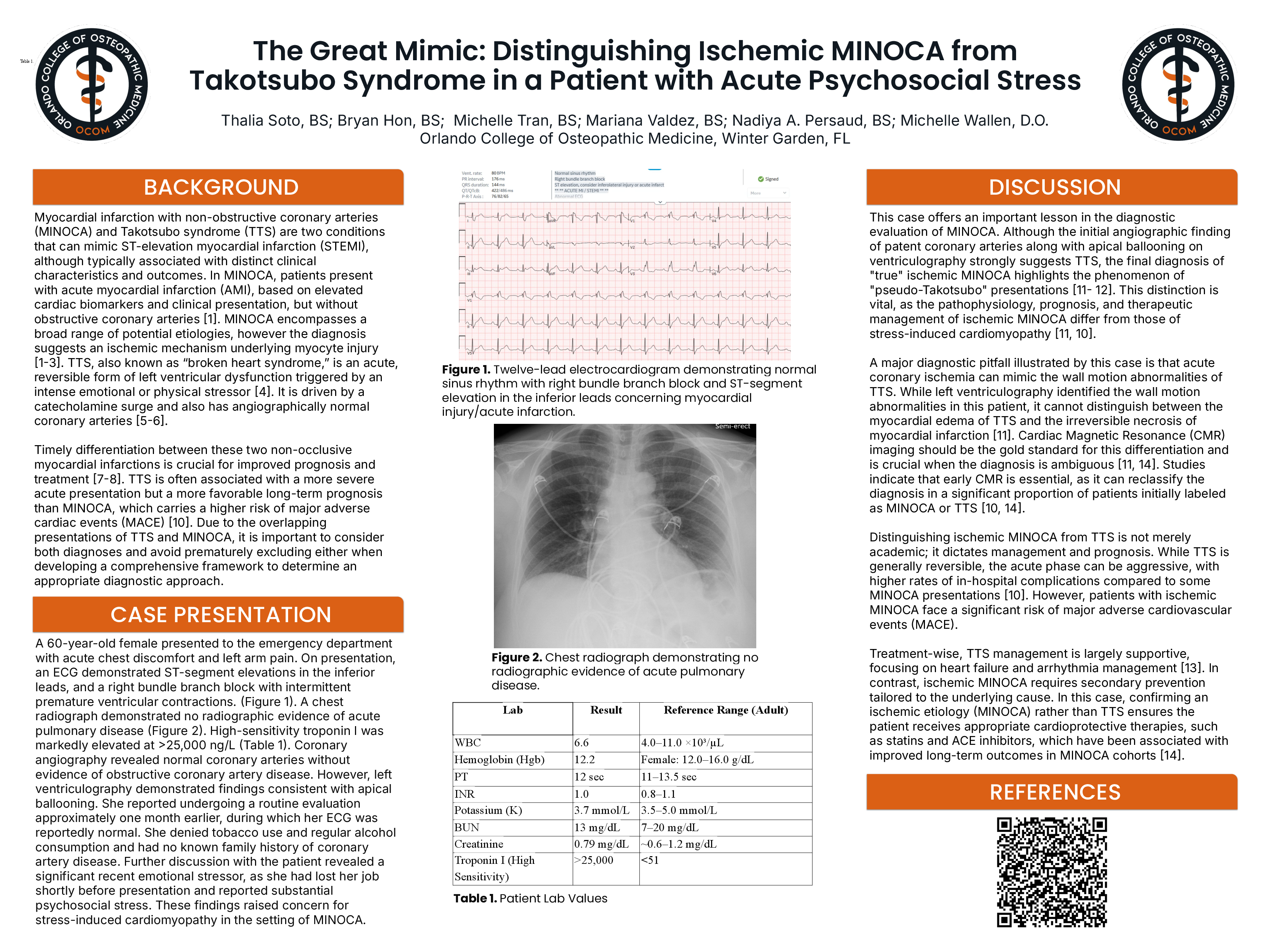
This report describes a 60-year-old female with no family history of coronary artery disease (CAD) who presented to the emergency department with acute chest discomfort and left-arm pain. Initial evaluation revealed ST elevation on inferior leads, markedly elevated high-sensitivity troponin levels greater than 25,000 ng/L, and non-obstructed coronary arteries on a coronary angiography. A left ventriculography also showed findings of apical ballooning. It was revealed that she recently underwent significant emotional stress, as she lost her job soon before presentation of symptoms.
DISCUSSION
Initially, this case appeared to be TTS rather than MINOCA, given the emotional trigger and left ventricular wall abnormalities. However, it is critical to consider that acute emotional stress can precipitate ischemic events and that acute coronary ischemia has the potential to mimic the wall motion abnormalities of TTS. Because MINOCA has a worse prognosis and a higher probability of major adverse cardiac events (MACE) compared to TTS, acknowledging the overlapping presentations of TTS and ischemic MINOCA can prevent early elimination of MINOCA from the differential diagnosis and develop a more comprehensive framework for the management of the appropriate diagnosis. This case underscores the importance of distinguishing between TTS and MINOCA, such as the utilization of Cardiac Magnetic Resonance (CMR) as the gold standard for the differentiation of myocardial edema of TTS and the necrosis of an MI, to optimize treatment and outcomes.