Abstract
Background:
Systemic Lupus Erythematosus (SLE) is an autoimmune disease characterized by the presence of pathogenic autoantibodies targeting nuclear and cellular components which drive tissue damage, chronic systemic inflammation, and heterogeneous clinical manifestations associated with significant morbidity and mortality[1]. Despite progress in the therapeutic management of SLE-associated co-morbidities, the risk of atherosclerotic cardiovascular disease (ASCVD) remains significantly increased in SLE patients, with reported risk of cardiac events at least two times higher and up to 50 times higher compared to age-matched healthy people[2]. Despite unique ASCVD pathways in SLE, treatment lacks specific targeting[2]. While shared medical decision making (SMD) reduces clinical flares, subclinical inflammation persists[2-5]. Notably, recent research validated the benefit of colchicine, the first anti-inflammatory drug approved for prevention of ASCVD in patients with residual inflammation[6,7,8] Here, we aim to highlight current evidence supporting a proposed benefit of colchicine for ASCVD prevention in SLE patients.
Methods:
A systematic search was conducted in March 2026 across PubMed. Terms searched were Systemic Lupus Erythematosus, Lupus, Cardiovascular, Cardiac, Atherosclerosis, Myocarditis, Pericarditis, Heart Disease, Colchicine.
Results:
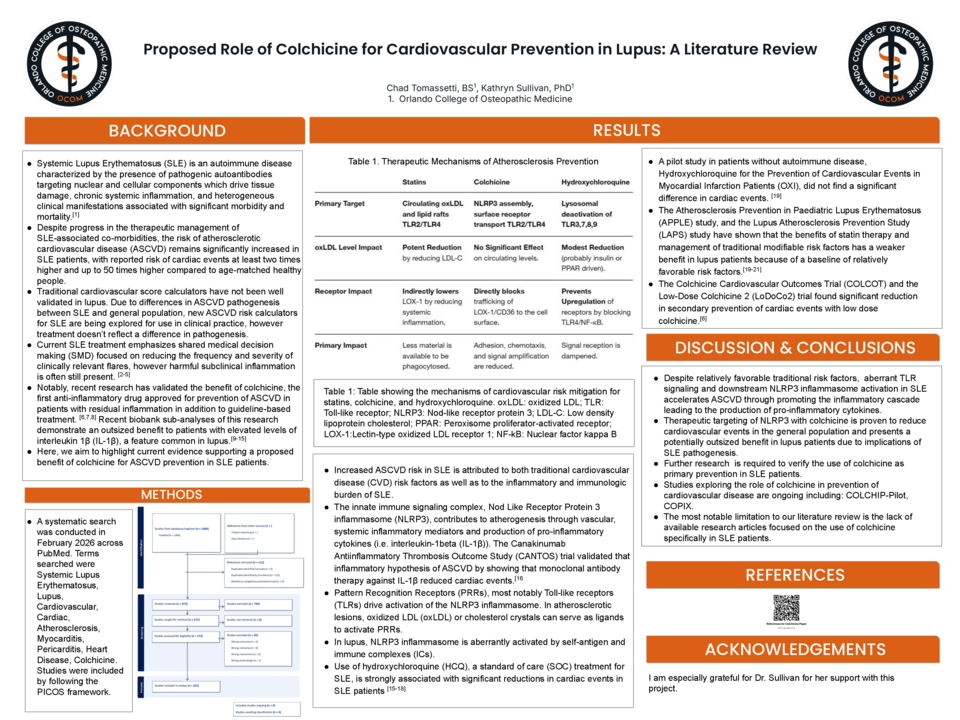
Increased ASCVD risk in SLE stems from both traditional risk factors and the disease's inflammatory burden[4]. The NLRP3 inflammasome drives atherogenesis via pro-inflammatory cytokines, a mechanism validated by the CANTOS trial[16]. In SLE, this inflammasome is aberrantly activated by self-antigens and immune complexes. While hydroxychloroquine (HCQ) significantly reduces cardiac events in lupus patients, it showed no such benefit in a pilot study of non-SLE patients.[15-18] Conversely, the APPLE and LAPS studies indicate that statins and traditional risk management are less effective in SLE due to relatively favorable baseline risk factors.[19-21] However, the COLCOT and LoDoCo2 trials demonstrated that low-dose colchicine significantly reduces secondary cardiac events.[6]
Discussion:
Despite relatively favorable traditional risk factors, aberrant NLRP3 inflammasome activation in SLE accelerates ASCVD through promoting the inflammatory cascade leading to the production of pro-inflammatory cytokines.Therapeutic targeting of NLRP3 with colchicine is proven to reduce cardiovascular events in the general population and presents a potentially outsized benefit in lupus patients due to implications of SLE pathogenesis.
Further research is required to verify the use of colchicine as primary prevention in SLE patients. Studies exploring the role of colchicine in prevention of cardiovascular disease are ongoing including: COLCHIP-Pilot, COPIX. The most notable limitation to our literature review is the lack of available research articles focused on the use of colchicine specifically in SLE patients.



