Abstract
Background
End-stage renal disease (ESRD) is the terminal stage of chronic kidney failure, defined by a glomerular filtration rate below 15 mL/min/1.73 m² for more than three months. It most commonly results from diabetes or hypertension in older adults; however, younger patients may develop ESRD from undiagnosed renal diseases such as glomerulonephritis. Chronic glomerulonephritis involves persistent inflammation of the glomeruli that can lead to fibrosis, cortical thinning, and renal atrophy. Early recognition is critical to prevent progression to ESRD. We report a case of a previously healthy 21-year-old male presenting with severe uremia and bilateral renal atrophy likely secondary to chronic undiagnosed glomerulonephritis.
Case Presentation
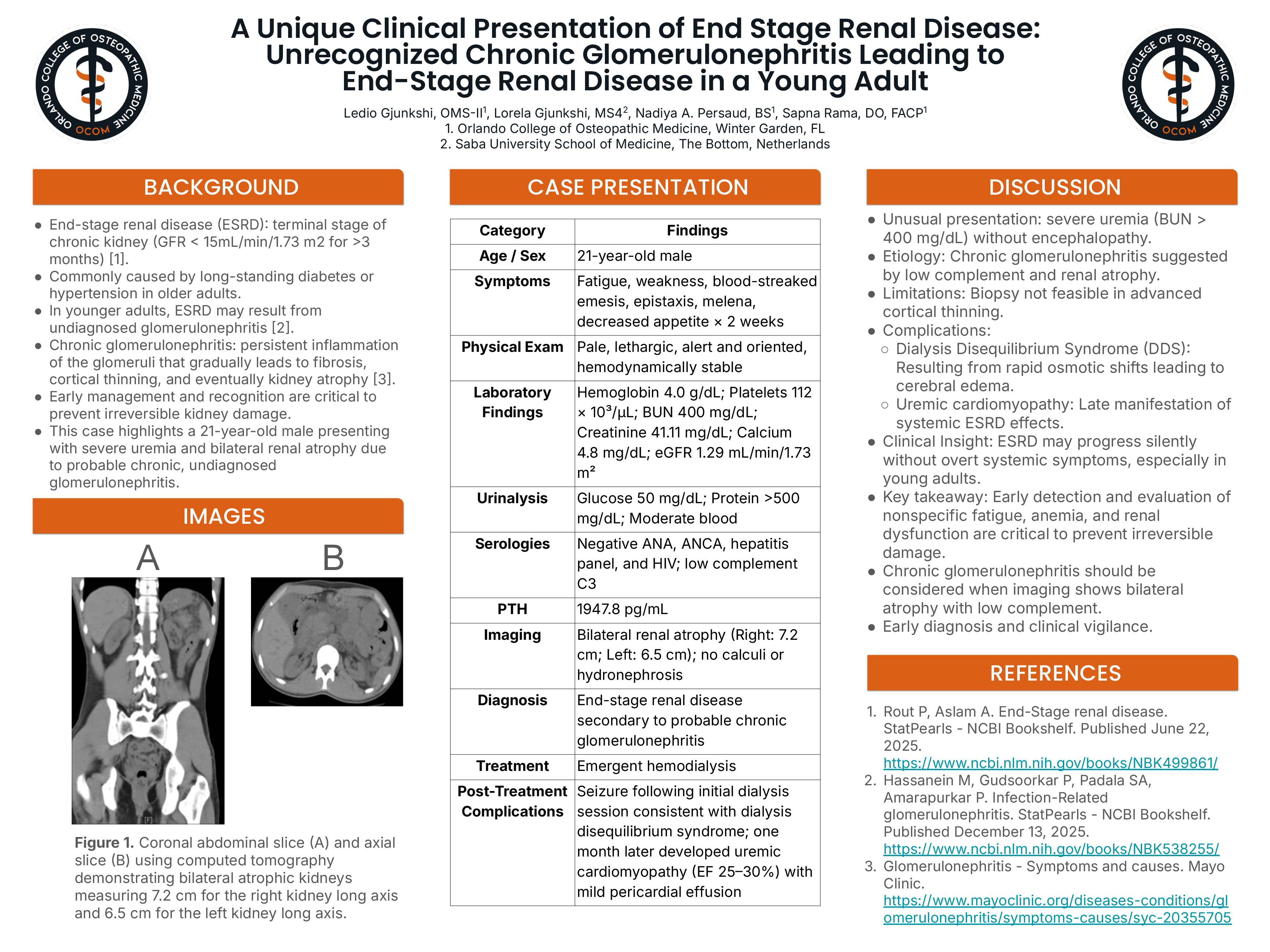
A 21-year-old male with no significant medical history presented with two weeks of fatigue, weakness, blood-streaked emesis, epistaxis, melena, and poor appetite. On admission he appeared pale and lethargic but was alert and oriented with stable vital signs. Laboratory evaluation revealed hemoglobin 4.0 g/dL, platelets 112 × 10³/µL, blood urea nitrogen (BUN) 400 mg/dL, creatinine 41.11 mg/dL, calcium 4.8 mg/dL, and an estimated glomerular filtration rate of 1.29 mL/min/1.73 m². Imaging demonstrated bilateral renal atrophy (right kidney 7.2 cm; left kidney 6.5 cm) without calculi or hydronephrosis. Urinalysis showed glucosuria, significant proteinuria, and hematuria. Parathyroid hormone was markedly elevated at 1947.8 pg/mL with an anion-gap metabolic acidosis. Serologic testing for ANA, ANCA, hepatitis, and HIV was negative, but complement C3 was reduced, raising suspicion for chronic glomerulonephritis. The patient underwent emergent hemodialysis and received blood transfusions. After the initial dialysis session he developed a seizure consistent with dialysis disequilibrium syndrome. Following stabilization and dialysis planning, he was discharged. One month later he returned with dyspnea and was diagnosed with uremic cardiomyopathy with an ejection fraction of 25–30% and mild pericardial effusion.
Discussion
This case demonstrates an atypical presentation of ESRD in a young adult with profound uremia but limited neurologic symptoms. Despite a BUN exceeding 400 mg/dL, the patient lacked significant encephalopathy, highlighting the variable presentation of ESRD. Chronic glomerulonephritis was the most likely etiology given reduced complement levels and renal atrophy on imaging. In advanced disease, renal biopsy is often impractical and management focuses on renal replacement therapy. Dialysis disequilibrium syndrome illustrates the risks of initiating dialysis in profoundly uremic patients due to rapid osmotic shifts causing cerebral edema. The subsequent development of uremic cardiomyopathy further demonstrates the systemic burden of ESRD and the importance of early diagnosis and transplant evaluation in young patients.