Abstract
Background: Ketamine and etomidate represent fundamentally different approaches to anesthesia induction, with traditional teaching emphasizing etomidate's hemodynamic stability and ketamine's sympathomimetic properties. However, real-world comparative safety data remain limited. We conducted a comprehensive pharmacovigilance analysis to characterize the cardiovascular and systemic safety profiles of these agents.
Methods: We analyzed the FDA Adverse Event Reporting System (FAERS) database from 2015 Q1 through 2025 Q3, restricting analysis to anesthesia-related indications. Adverse events were classified using MedDRA terminology. Disproportionality analysis employed six complementary metrics: Reporting Odds Ratio (ROR), Proportional Reporting Ratio (PRR), Bayesian Confidence Propagation Neural Network (IC), Multi-item Gamma Poisson Shrinkage (EBGM), chi-squared test, and linear regression. Signals were considered significant when ROR >2 with 95% CI lower bound >1.
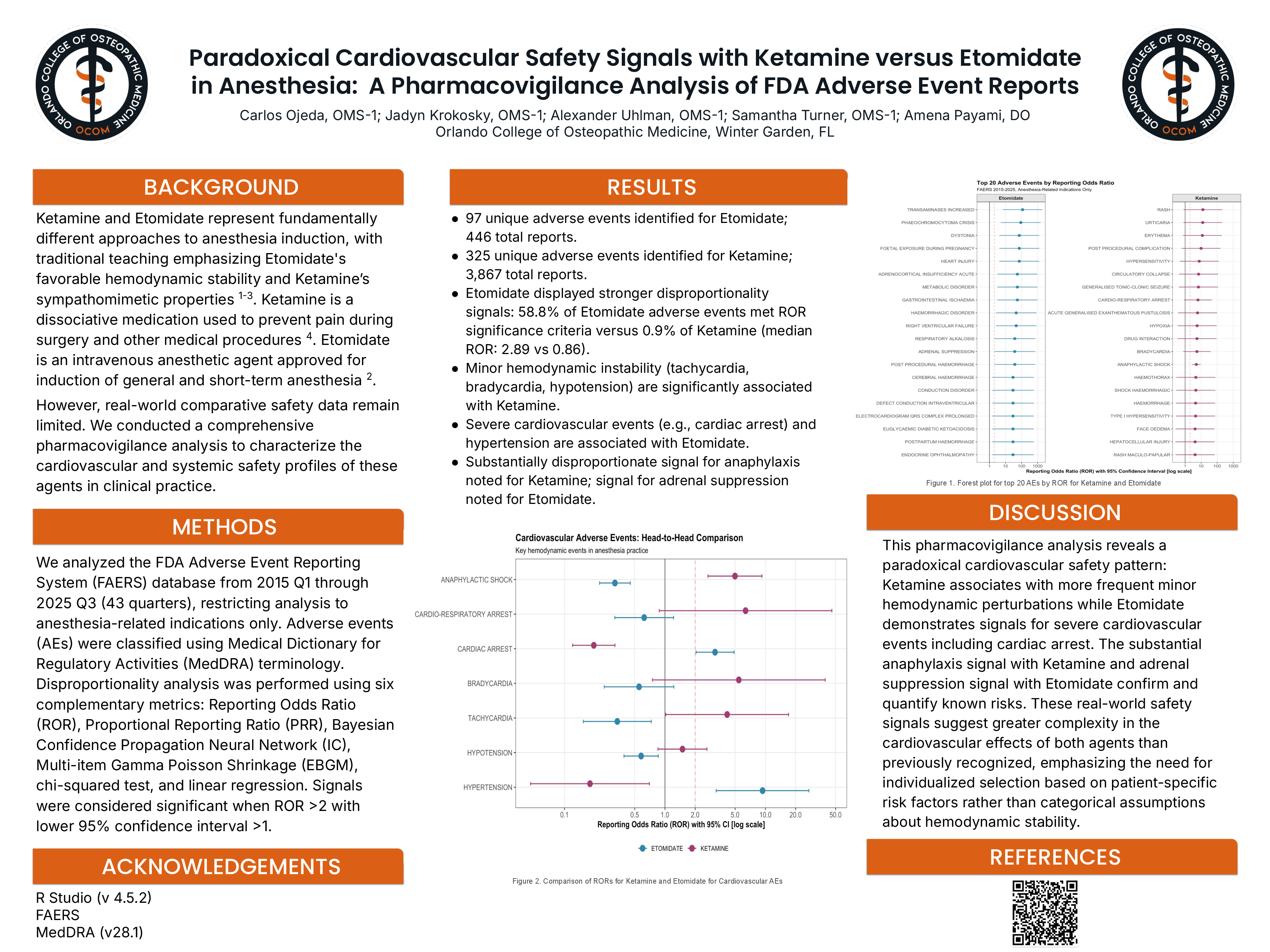
Results: We identified 97 unique adverse events for etomidate (446 reports) and 325 for ketamine (3,867 reports). Despite fewer reports, etomidate demonstrated substantially stronger disproportionality signals: 58.8% of events met ROR significance threshold versus 0.9% for ketamine (median ROR 2.89 vs 0.86).
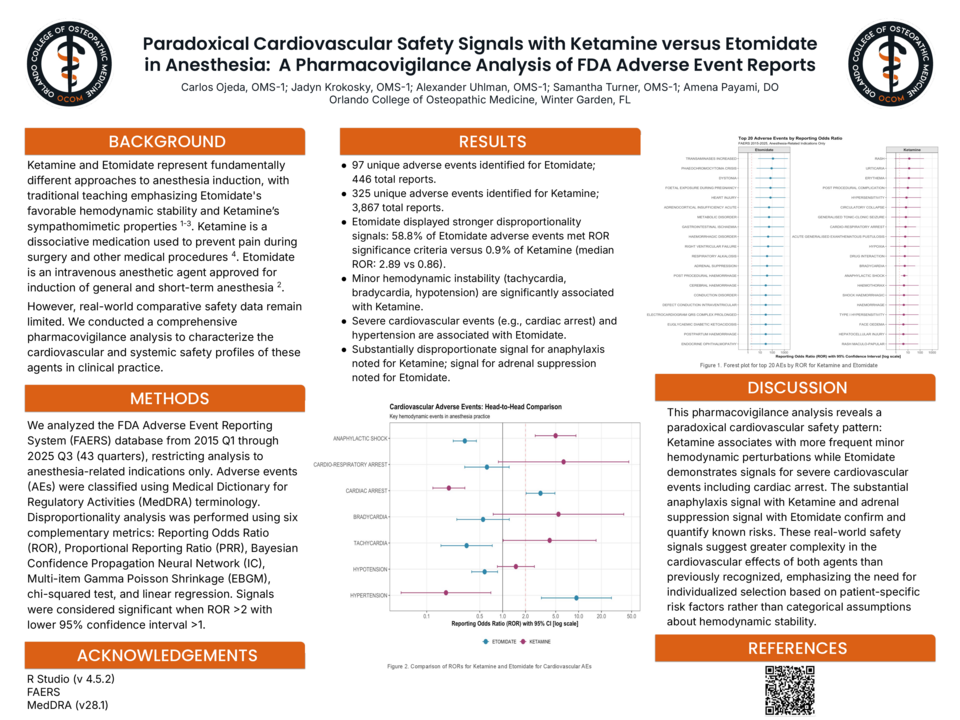
A paradoxical cardiovascular pattern emerged. Minor hemodynamic instability associated with ketamine: tachycardia (ROR 4.16 [95% CI 2.56-6.76]), bradycardia (ROR 5.44 [3.68-8.05]), and hypotension (ROR 1.49 [1.35-1.66]). Conversely, etomidate showed signals for severe events: cardiac arrest (ROR 3.15 [2.26-4.40]) and hypertension (ROR 9.37 [5.04-17.44]).
Ketamine demonstrated substantial anaphylaxis signal (ROR 4.98 [4.58-5.41], 561 reports) versus etomidate (ROR 0.32 [0.23-0.44], 38 reports). Etomidate-specific signals included adrenal suppression (ROR 37.76 [13.96-102.13]), malignant hyperthermia (ROR 13.00 [8.17-20.70]), and dystonia (ROR 72.03 [33.11-156.76]).
Conclusions: This pharmacovigilance analysis reveals a paradoxical cardiovascular pattern: ketamine associates with frequent minor hemodynamic perturbations while etomidate demonstrates severe cardiovascular event signals including cardiac arrest. The substantial anaphylaxis signal with ketamine and adrenal suppression with etomidate quantify known risks. These findings suggest greater complexity than traditional teaching recognizes, emphasizing individualized agent selection based on patient-specific risk factors.