Abstract
Introduction/Objective:
Creatine monohydrate is a widely used dietary supplement for performance enhancement in sports [1]. Although its efficacy and safety are well established in adults, creatine use among adolescents remains controversial [2]. Existing literature often extrapolates adult data to younger populations and prioritizes performance outcomes, with limited emphasis on safety monitoring, dosing strategies, and patient counseling [3]. Inconsistent definitions of “athlete” and limited adolescent representation further restrict clinical applicability [3]. This systematic review aimed to evaluate the safety of creatine monohydrate supplementation in adolescent athletes and physically active youth.
Methods:
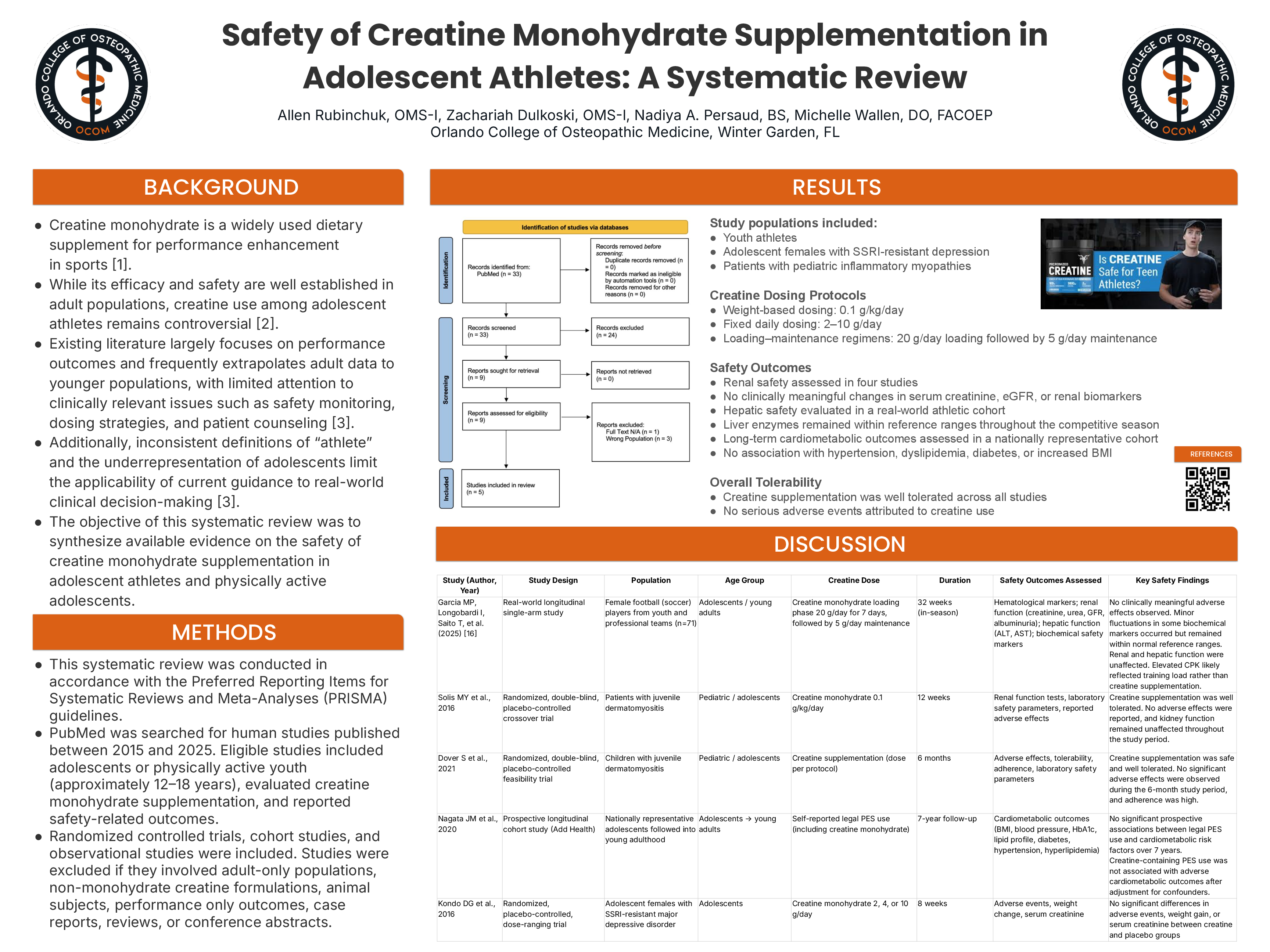
This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. PubMed was searched for human studies published between 2015 and 2025. Eligible studies included adolescents or physically active youth (approximately 12–18 years), evaluated creatine monohydrate supplementation, and reported safety-related outcomes. Randomized controlled trials, cohort studies, and observational studies were included. Studies involving adult-only populations, non-monohydrate creatine formulations, animal subjects, performance-only outcomes, case reports, reviews, or conference abstracts were excluded.
Results:
Five studies met inclusion criteria, including pediatric, adolescent, and young adult populations such as youth athletes, adolescent females with SSRI-resistant depression, and patients with pediatric inflammatory myopathies. Creatine dosing regimens ranged from weight-based protocols (0.1 g/kg/day) to fixed daily doses (2–10 g/day) and loading–maintenance strategies (20 g/day loading followed by 5 g/day maintenance). Study durations ranged from 8 to 32 weeks, with one cohort followed for seven years. Renal safety was evaluated in four studies, with no clinically meaningful changes in serum creatinine, estimated glomerular filtration rate, or other renal biomarkers. Hepatic safety assessed in an athletic cohort showed liver enzymes remained within reference ranges. Long-term cardiometabolic outcomes demonstrated no association between adolescent creatine-containing supplement use and hypertension, dyslipidemia, diabetes, or increased body mass index. No serious adverse events were attributed to creatine supplementation.
Conclusions:
Current evidence suggests that creatine monohydrate supplementation is not associated with clinically meaningful renal, hepatic, or cardiometabolic safety concerns in adolescent and physically active youth. However, limited adolescent-specific data and population heterogeneity remain significant gaps. Future studies should prioritize adolescent-focused trials with standardized dosing and safety monitoring to guide clinical counseling and evidence-based recommendations.