Abstract
Introduction:
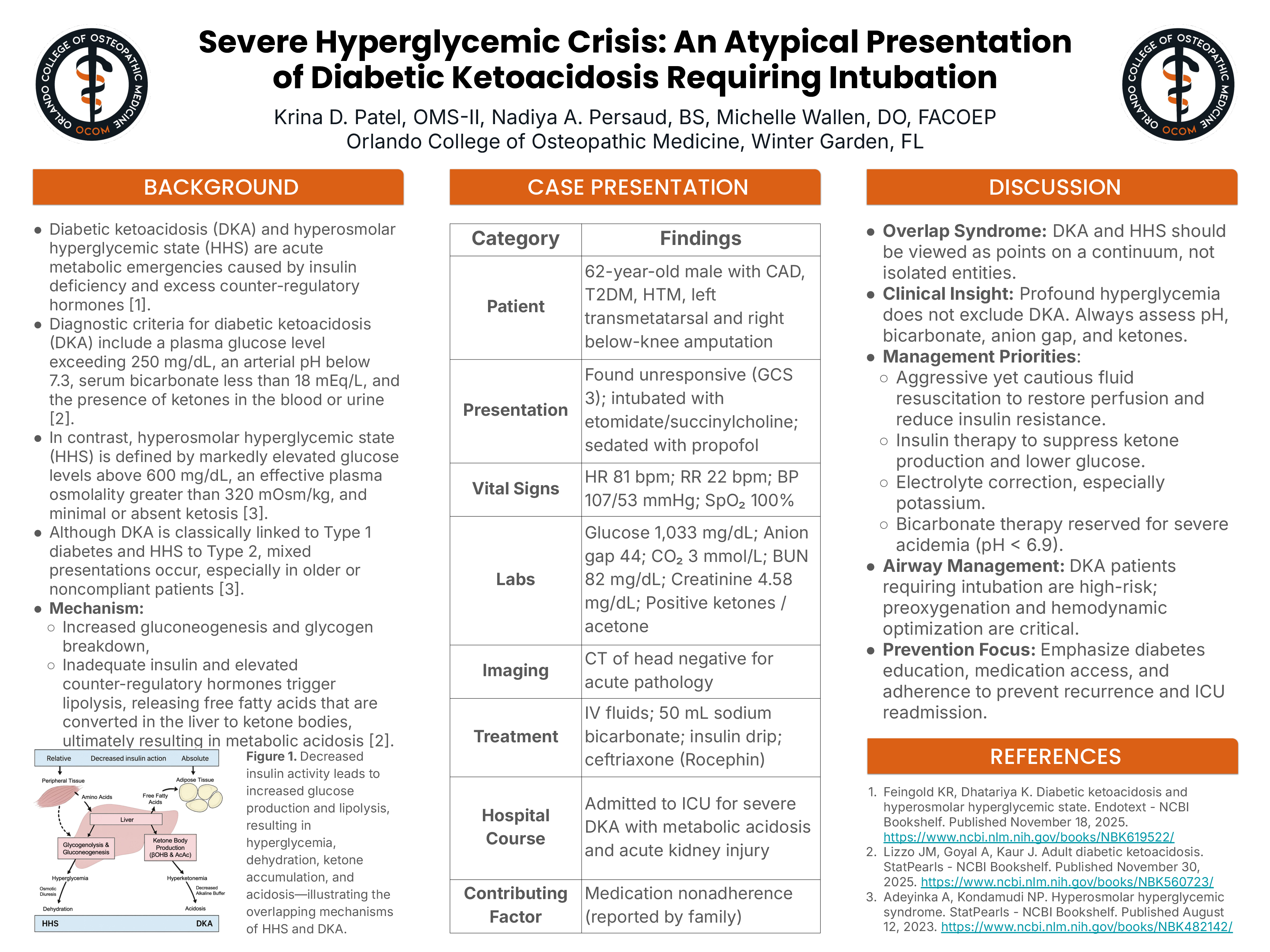
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are acute metabolic emergencies associated with uncontrolled diabetes mellitus and excess counterregulatory hormones, including glucagon, cortisol, catecholamines, and growth hormone. Although they share underlying pathophysiology, they differ in biochemical and clinical features. DKA, classically associated with type I diabetes mellitus, is characterized by hyperglycemia, ketosis, and metabolic acidosis, whereas HHS typically presents with severe hyperglycemia and hyperosmolarity with minimal ketosis in patients with type II diabetes mellitus (T2DM). Increasing evidence suggests these conditions may coexist, particularly in older individuals with uncontrolled T2DM or precipitating stressors such as infection, myocardial infarction, or medication nonadherence. This case highlights an overlapping presentation of DKA and HHS.
Case Presentation:
A 62-year-old male with a history of coronary artery disease, T2DM, hypertension, left transmetatarsal amputation, and right below-knee amputation was brought to the emergency department unresponsive with a Glasgow Coma Scale score of 3. He was immediately intubated using etomidate and succinylcholine, with correct endotracheal tube placement confirmed by bilateral breath sounds, CO₂ monitoring, and chest radiography. Propofol was initiated for sedation. Point-of-care glucose read “high,” raising concern for a hyperglycemic crisis.
Vital signs included heart rate 81 bpm, respiratory rate 22 bpm, blood pressure 107/53 mmHg, and SpO₂ 100%. Despite not meeting full systemic inflammatory response syndrome criteria, a sepsis alert was activated due to severity of illness. Intravenous fluids and ceftriaxone were initiated. Laboratory studies revealed a white blood cell count of 11.7 ×10³/µL, hemoglobin 9.3 g/dL, platelets 323 ×10³/µL, blood urea nitrogen 82 mg/dL, creatinine 4.58 mg/dL, anion gap 44, CO₂ 3 mmol/L, positive acetone, and serum glucose 1,033 mg/dL.
The patient received intravenous sodium bicarbonate, aggressive fluid resuscitation, and was started on an insulin infusion. A non-contrast CT of the head showed no acute intracranial pathology. He was admitted to the intensive care unit for management of severe DKA, metabolic acidosis, and acute kidney injury. No infectious source was identified; however, family later reported significant medication nonadherence, likely precipitating the hyperglycemic crisis.
Discussion:
This case underscores three key clinical considerations: hyperglycemic crises exist along a continuum rather than as discrete entities; markedly elevated serum glucose does not exclude DKA; and prevention through patient education, medication access, and adherence support is critical. Early recognition and prompt management remain essential to improving outcomes and preventing life-threatening complications.