Abstract
Background: The 2023-2024 RSV season marked the first availability of the monoclonal antibody nirsevimab for passive immunoprophylaxis against RSV infection among young infants. Limited information was available on the anticipated uptake of nirsevimab administration.
Design/Methods: We performed a retrospective chart review of infants eligible to receive RSV immunoprophylaxis during the 2023-2024 RSV season. Pearson’s chi-square tests were performed to compare demographics and childhood vaccine uptake by nirsevimab status.
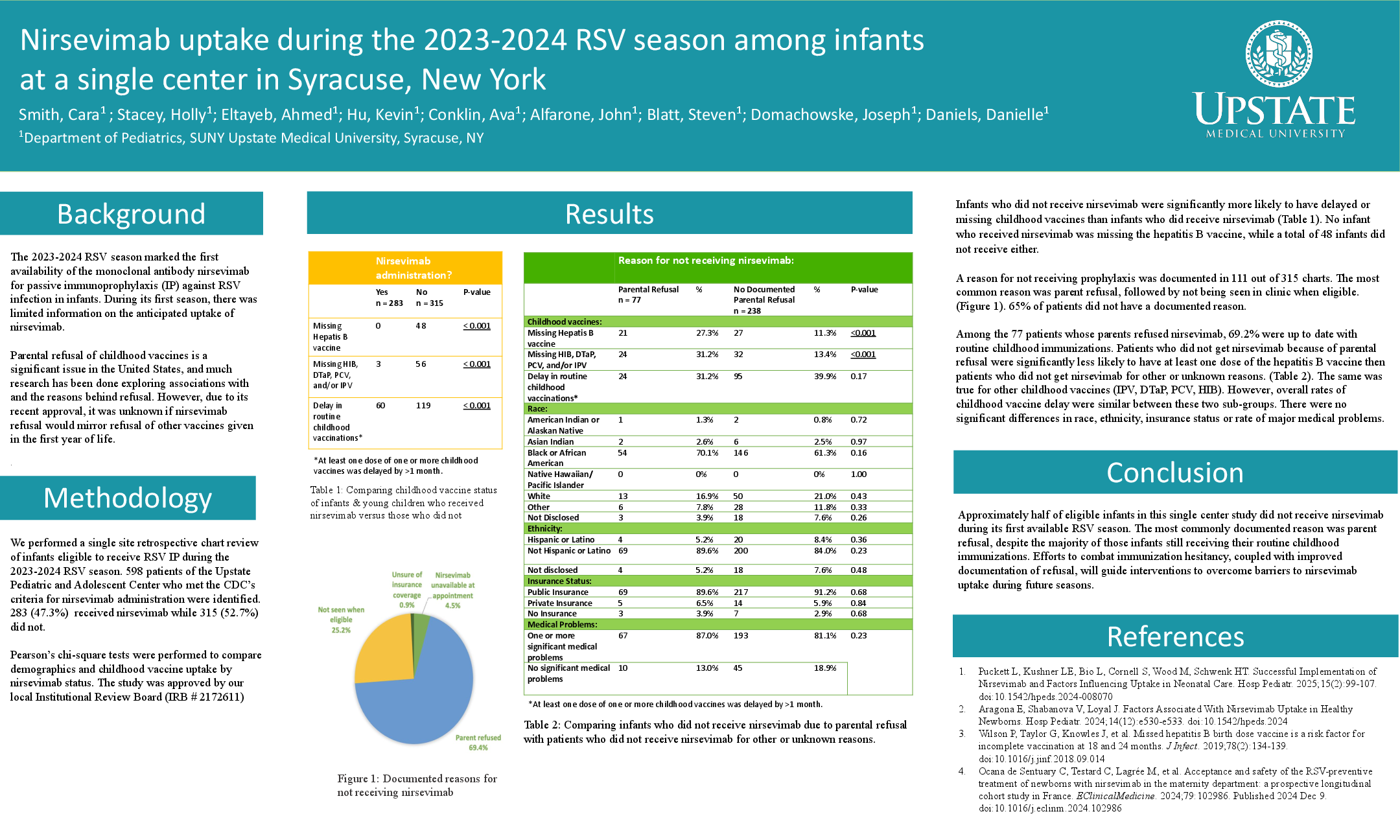
Results: We identified 598 patients who were eligible to receive RSV IP. Of these, 315 did not receive nirsevimab. These infants were significantly more likely to have delayed or missing childhood vaccines (35.56%) than those who did receive nirsevimab (21.20%) (p = 0.0001). All infants who received nirsevimab received the Hepatitis B vaccine, compared to 48 infants who did not receive either.
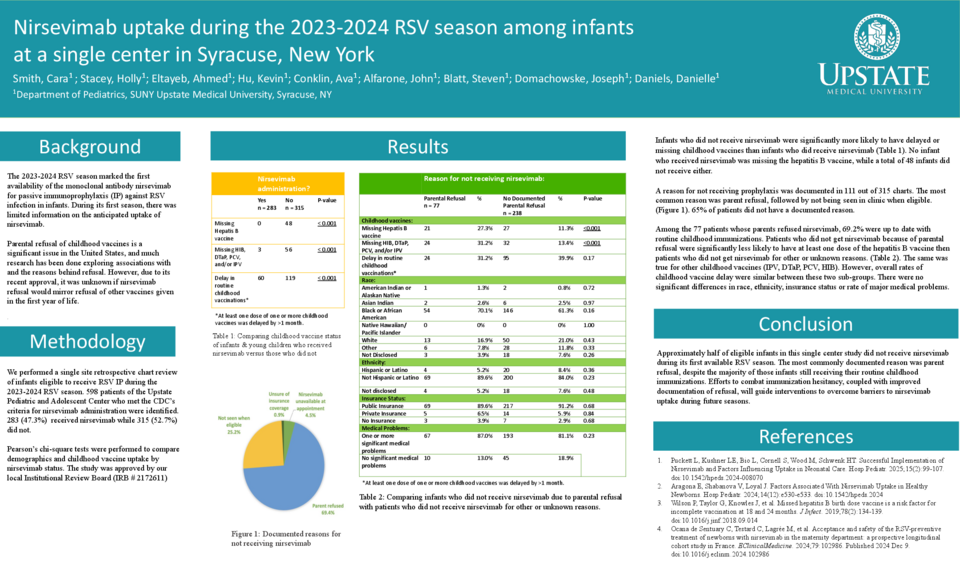
A reason for not receiving prophylaxis was documented in 111 out of 315 charts. The most common reasons were parent refusal (69.4%), not seen at clinic when eligible (25.2%), vaccine unavailable at appointment (4.5%) and unsure of insurance coverage (0.9%).
Patients who did not get nirsevimab because of parental refusal were significantly less likely to have at least one dose of the Hepatitis B vaccine then patients who did not get nirsevimab for other/unknown reasons. This was true for other childhood vaccines (IPV, DTaP, PCV, HIB). However, overall rates of childhood vaccine delay were similar between these two sub-groups (p = 0.1688). There were no significant differences in race, ethnicity, insurance status or rate of major medical problems.
Conclusion: Approximately half of eligible infants in this study did not receive nirsevimab during its first available RSV season. The most documented reason was parent refusal, despite most of those infants receiving other routine immunizations. Efforts to combat immunization hesitancy, coupled with improved documentation of refusal, will guide interventions to overcome barriers to nirsevimab uptake during future seasons.