Abstract
Background:
The transition from pediatric to adult care – typically occurring between ages 18-21 - for patients with renal dysfunction, including chronic kidney disease or End-Stage Renal Disease, is a vulnerable time and warrants careful planning between the patient and their pediatric and adult provider. Transitioning from a family-centered approach in pediatric care to a patient-centered approach in adult care may pose challenges for patients, including psychological stress and increased healthcare costs. A lack of proper transition planning can lead to knowledge gaps for patients in terms of treatment, medication noncompliance, and a lack of follow-up appointments. These effects can lead to negative outcomes for patients, including a decline in renal function or loss of graft, leading to higher hospitalizations and poor long-term outcomes.
Methods
We retrospectively analyzed publicly available data from the United States Renal Data System (USRDS) annual data for patients with End-Stage Renal Disease. Patients were stratified into pediatric age subgroups (0-4, 5-9, 10-13, 14-17) and adolescents (18-21). Outcomes evaluated include dialysis modality (in-center hemodialysis, home hemodialysis, peritoneal dialysis, or transplant), in addition to hospitalizations (Admissions per 1,000 patient-years), and mortality (deaths per 1,000 patient-years). Since the USRDS database reported mortality and hospitalization as a broader age range (18-29), this subgroup was used as a proxy for adolescents 18-21 undergoing transition. Patients outside this age range were excluded from further analysis.
Results:
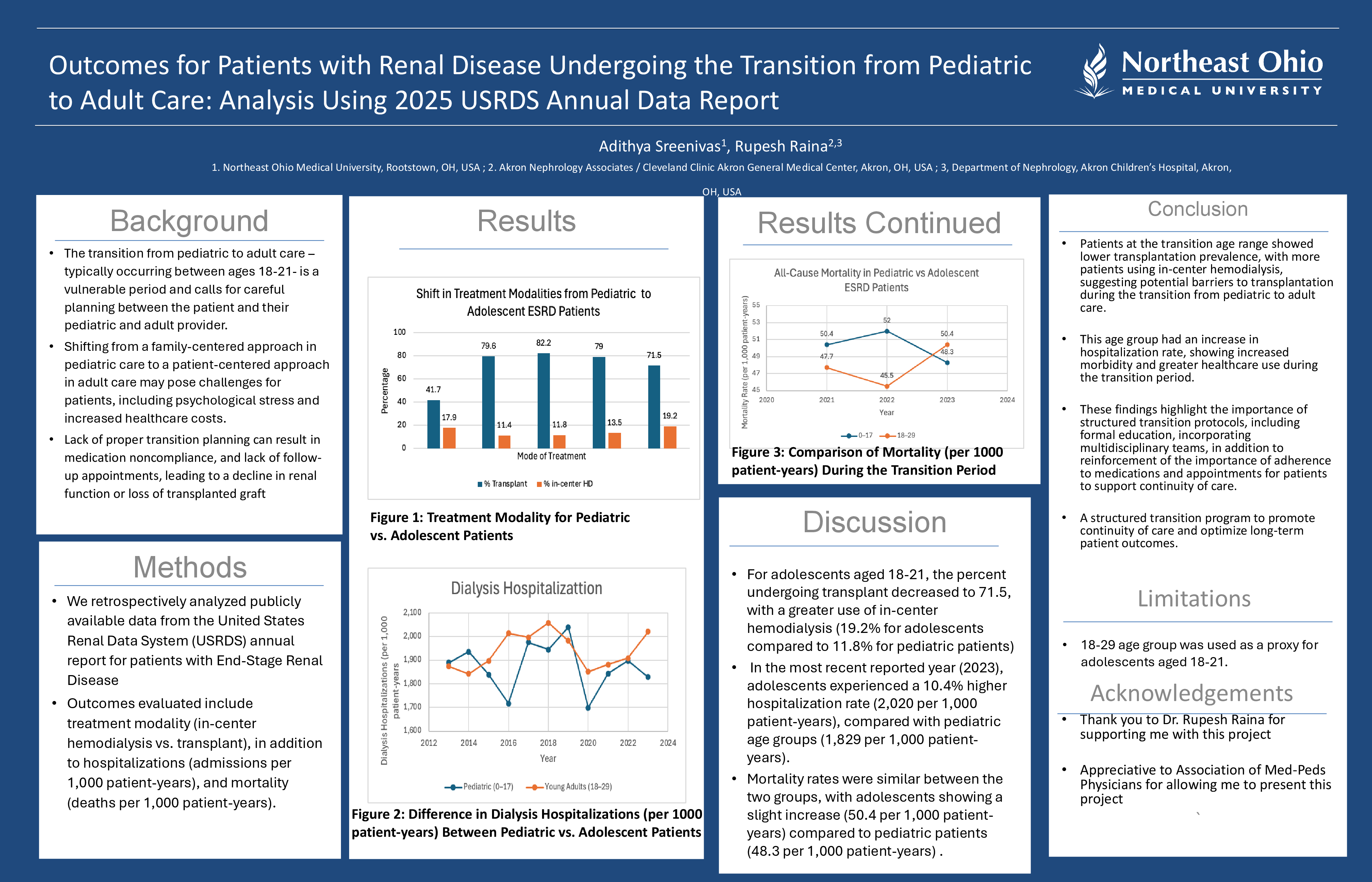
For pediatric patients, kidney transplantation was the predominant treatment modality (79%). For adolescents aged 18-21, the percent undergoing transplant decreased to 71.5, with a greater utilization of in-center hemodialysis (19.2% for adolescents compared to 11.8% for pediatric patients). In the most recent reported year (2023), adolescents experienced a 10.4% higher hospitalization rate (2,020 per 1,000 patient-years), compared with pediatric age groups (1,829 per 1,000 patient-years). Mortality rates were similar between the two groups, with adolescents showing a slight increase (50.4 per 1,000 patient-years) compared to (48.3 per 1,000 patient-years) for pediatric patients. These findings suggest potential barriers to treatment continuity for adolescents undergoing the transition of care to adult nephrology.
Conclusion:
Patients at the transition age range demonstrated lower transplantation prevalence, with more patients utilizing in-center hemodialysis, suggesting potential barriers to transplantation during the transition from pediatric to adult care. This age group had an increase in hospitalization rate, indicating increased morbidity and greater healthcare utilization during this period. These findings highlight the importance of structured transition protocols, including formal education, incorporating multidisciplinary teams, in addition to reinforcement of the importance of adherence to medications and appointments for patients to support continuity of care. A limitation of this study is using the 18-29 age group as a proxy for adolescents aged 18-21. Overall, these findings underscore the need for a structured transition program to promote continuity of care and optimize long-term patient outcomes.