Abstract
Background: Transcatheter aortic valve replacement has emerged as the preferred low-risk alternative to surgical valve replacement for patients with severe aortic stenosis. Cardiac rehabilitation (CR) improves functional capacity post-TAVR, yet participation remains suboptimal. Patient education may represent a modifiable factor influencing engagement.
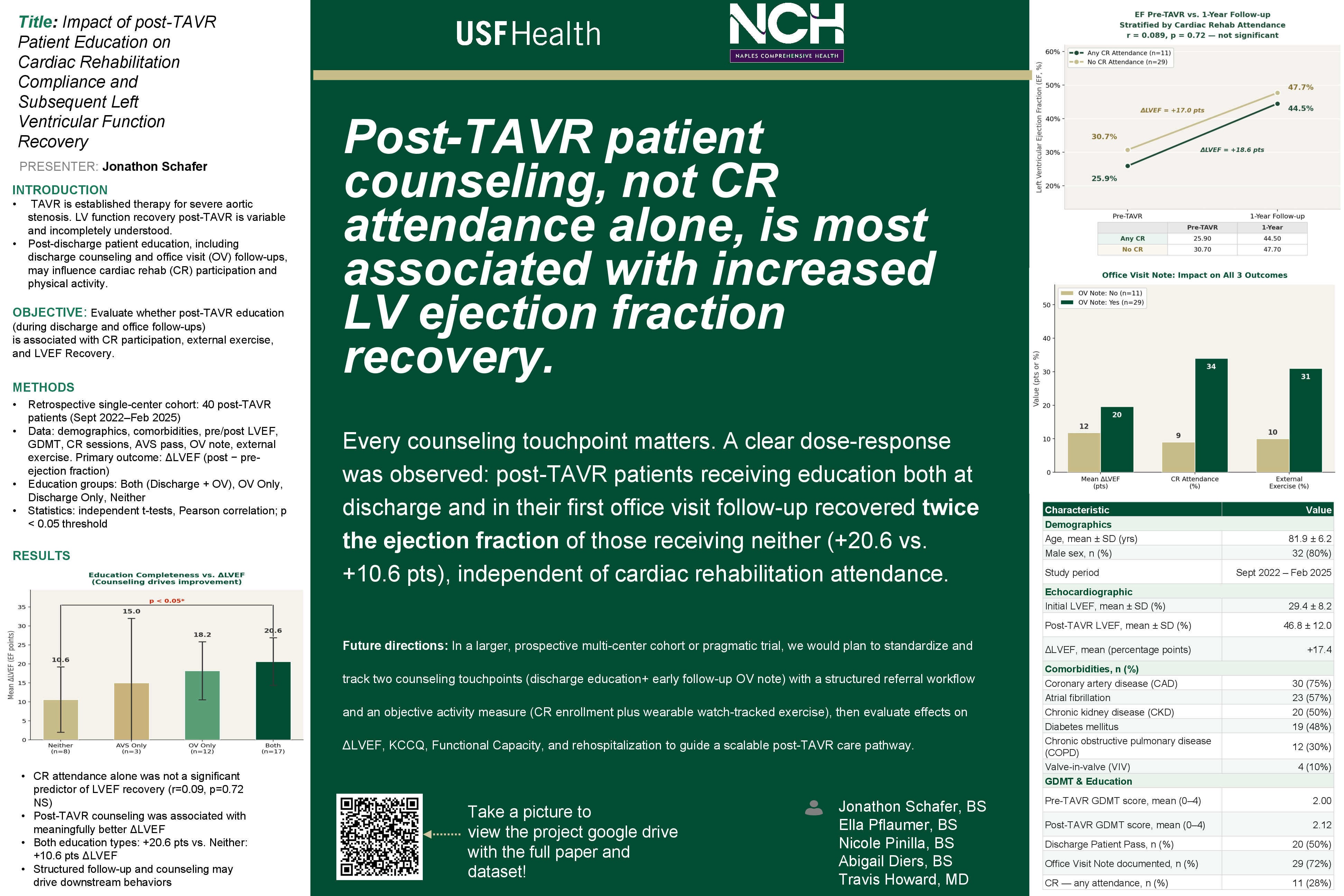
Methods: A retrospective cohort study of 40 patients who had undergone a TAVR was conducted. The patients chosen had a baseline left ventricular ejection fraction (LVEF) of < 40%. Documentation of structured patient education at discharge and during follow-up visits was assessed, and multivariable linear regression was used to evaluate predictors of ΔLVEF.
Results: Among 40 post-TAVR patients with reduced ejection fraction (mean baseline LVEF 29.4 ± 8.2%), mean ΔLVEF at one year was +17.4 percentage points (post-TAVR LVEF 46.8 ± 12.0%). CR attendance was low (28%) and was not associated with greater LVEF recovery (attendees: +18.6 ± 12.3 vs. non-attendees: +17.0 ± 13.5 percentage points; p = 0.72; r = 0.089). In contrast, documentation of CR education at the first post-procedural office visit was associated with greater ΔLVEF (+20.2 ± 12.0 vs. +12.4 ± 13.4 percentage points; difference +7.8; p = 0.075). A graded increase in ΔLVEF was observed across education groups: neither (n = 8, +10.6), discharge pass only (n = 3, +15.8), OV note only (n = 12, +18.8), and both (n = 17, +20.6). Office visit education was strongly associated with participation in any exercise modality, including CR, physical therapy, or home exercise (83% vs. 27%; p < 0.001).
Conclusions: In this cohort, there was not a clear relationship between CR attendance and increase in LVEF. Documentation of structured patient education, however, was independently associated with improved ventricular recovery following TAVR in exploratory analysis. These findings suggest that post-procedural engagement and counseling may contribute to favorable remodeling beyond mechanical relief of afterload. In multivariable regression, documented office visit counseling was independently associated with an 8.35 percentage-point greater ΔLVEF (95% CI 0.36–16.35; p = 0.041) after adjusting for baseline LVEF and CAD. Prospective studies are warranted to further evaluate this relationship.
References
- Pedersen CG, Nielsen CV, Lynggaard V, Zwisler AD, Maribo T. The patient education strategy “learning and coping” improves adherence to cardiac rehabilitation in primary healthcare settings: a pragmatic cluster-controlled trial. BMC Cardiovascular Disorders 2022;22. https://doi.org/10.1186/s12872-022-02774-8.
- Khan U, Abdelgalil MS, Khan MH, Ali J, Majeed Z, Amin AM, et al. Exercise-based cardiac rehabilitation after transcatheter aortic valve replacement: a systematic review and meta-analysis of randomized controlled trials. Future Cardiology 2026;22:155–66. https://doi.org/10.1080/14796678.2026.2615390.
- Mehdipoor G, Chen S, Chatterjee S, Torkian P, Ben-Yehuda O, Leon MB, et al. Cardiac structural changes after transcatheter aortic valve replacement: systematic review and meta-analysis of cardiovascular magnetic resonance studies. Journal of Cardiovascular Magnetic Resonance 2020;22. https://doi.org/10.1186/s12968-020-00629-9.
- Duan H, Zhang C, Zhang Q, Chen D, et al. Cardiac rehabilitation for TAVR patients: mechanisms, current status, and future directions. Frontiers in Cardiovascular Medicine 2025;12. https://doi.org/10.3389/fcvm.2025.1701764.