Abstract
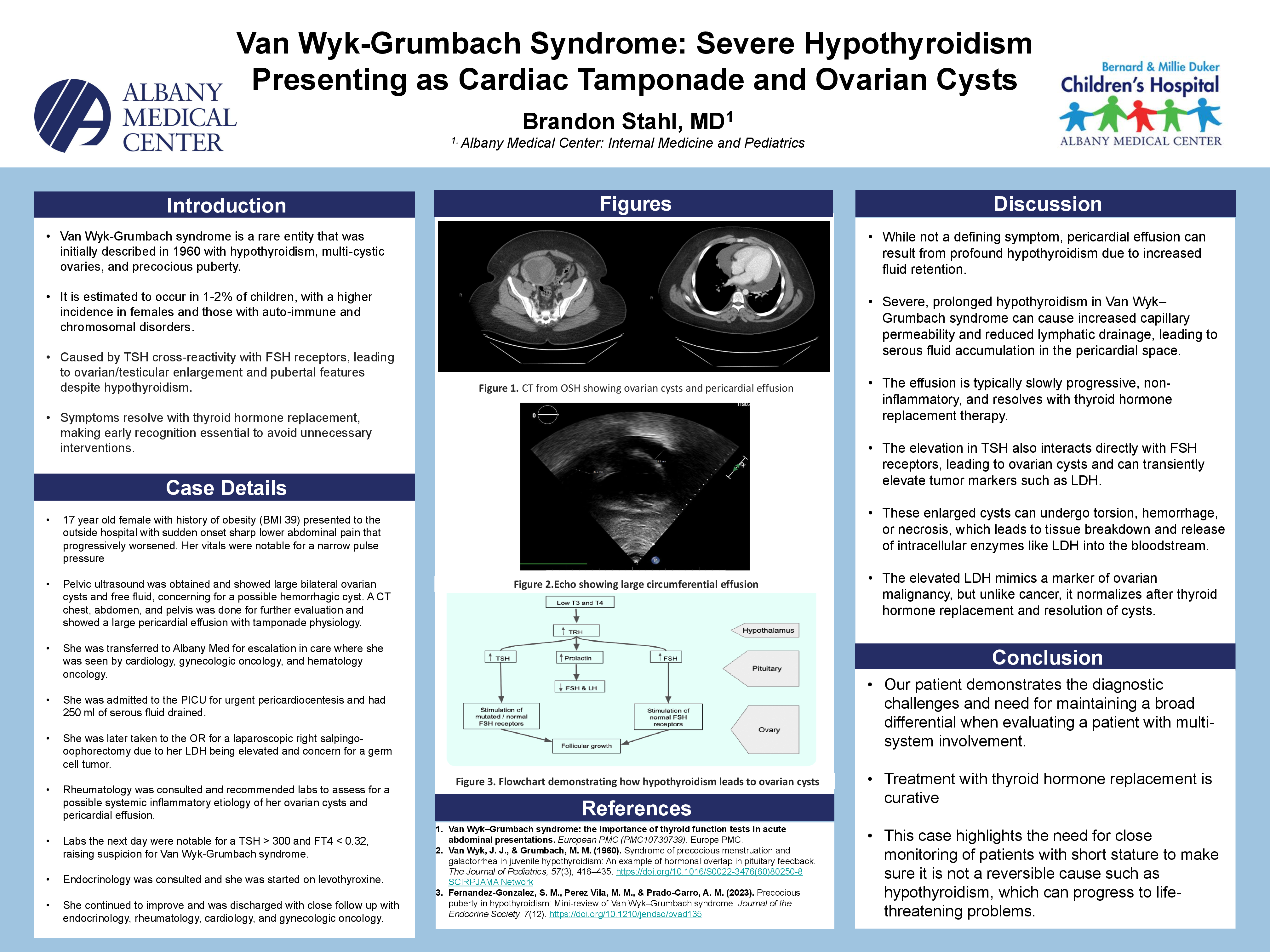
A 17-year-old female with a history of class 2 obesity (BMI 39) presented to an outside hospital initially with sudden onset sharp lower abdominal pain that progressively worsened. Pelvic ultrasound was obtained and showed large bilateral ovarian cysts and free fluid, concerning for a possible hemorrhagic cyst. Her vitals were notable for a narrow pulse pressure without tachycardia but were otherwise normal A CT chest, abdomen, and pelvis was done for further evaluation and showed a large pericardial effusion with tamponade physiology. She was transferred to Albany Med for escalation in care where she was seen by cardiology, gynecologic oncology, and hematology oncology. She was admitted to the PICU for urgent pericardiocentesis and had 250 ml of serous fluid drained. She was later taken to the OR with gyn-onc for a laparoscopic right salpingo-oophorectomy due to her LDH being elevated and concern for a germ cell tumor. Rheumatology was consulted and recommended labs to assess for a possible systemic inflammatory etiology of her ovarian cysts and pericardial effusion. Her labs the following day showed some mild electrolyte abnormalities but were most notable for a TSH > 300 and FT4 < 0.32, raising suspicion for Van Wyk-Grumbach syndrome. Endocrinology was consulted and she was started on levothyroxine. She continued to improve and was discharged with close follow up with endocrinology, rheumatology, cardiology, and gynecologic oncology.
Van Wyk-Grumbach syndrome is a rare entity that was initially described in 1960 with hypothyroidism, multi-cystic ovaries, and precocious puberty. It is estimated to occur in 1-2% of children, with a higher incidence in females and those with auto-immune and chromosomal disorders. While not a defining symptom, pericardial effusion can result from profound hypothyroidism due to increased fluid retention. The elevation in TSH also interacts directly with FSH receptors, leading to ovarian cysts and can transiently elevate tumor markers such as LDH. Our patient demonstrates the diagnostic challenges and need for maintaining a broad differential when evaluating a patient with multi-system involvement. This case highlights the need for close monitoring of patients with short stature to make sure it is not a reversible cause such as hypothyroidism, which can progress to life-threatening problems.