Abstract
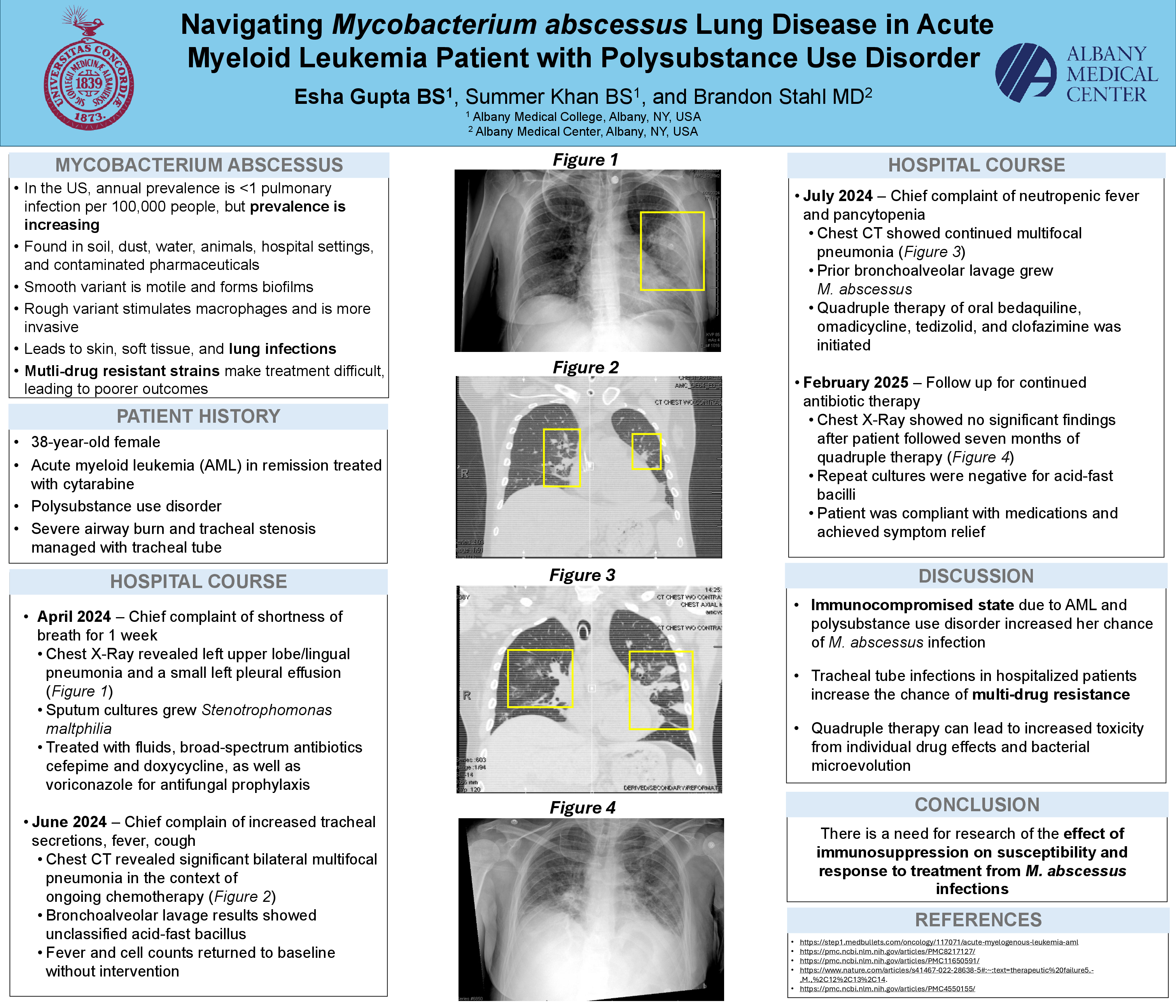
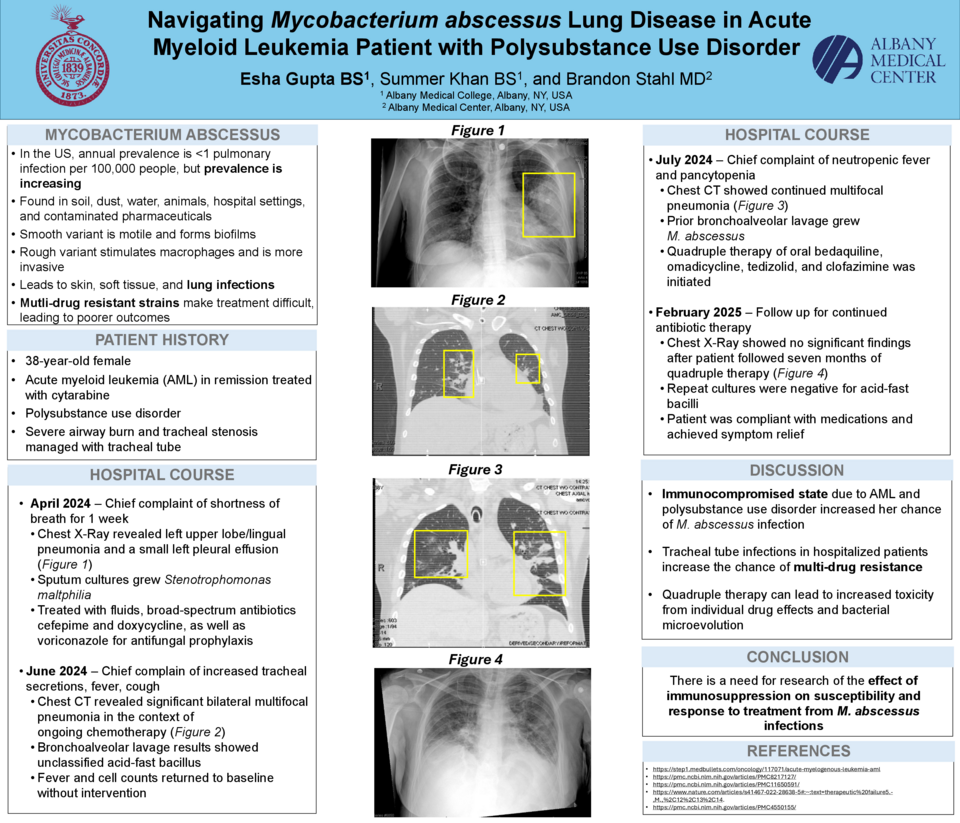
A 38-year-old female with a past medical history of acute myeloid leukemia (AML) treated with cytarabine, polysubstance use disorder, and severe airway burn managed with a tracheal tube presented to the ED with eight days of fever. Three months ago, the patient reported shortness of breath for a week. Chest X-ray showed left upper lobe/lingual pneumonia and a small left pleural effusion. Respiratory culture was positive for Stenotrophomonas maltiphilia growth. She was started on cefepime and antifungal prophylaxis. Two months later, the patient was admitted for chemotherapy when she began having increased tracheal secretions, fever, and cough. Chest CT showed bilateral multifocal pneumonia. Bronchoalveolar lavage results showed growth of an unclassified acid-fast bacillus that was M. tuberculosis negative and no antimicrobials were started. Subsequently, her fever came down, cell counts recovered, and she was discharged. One month later, the patient presented with neutropenic fevers and pancytopenia. Her cultures from her prior admission showed a multi-drug resistant Mycobacterium abscessus complex. Repeat cultures tested for drug sensitivities and she was started on a four drug regimen of oral bedaquiline, omadicycline, tedizolid, and clofazimine. After seven months of treatment, sputum culture and smear were negative for acid fast bacilli and chest X-ray showed improved findings.
Mycobacterium abscessus is a nontuberculous mycobacterium found in soil, dust, water, animals, hospital settings, and contaminated pharmaceuticals. A smooth variant produces glycopeptidolipid-containing biofilms to evade innate immune defenses, while a rough variant stimulates macrophages to cause more severe lung disease. M. abscessus causes skin and soft tissue infections as well as lung infections, especially in those with pre-existing lung disease. The patient’s history of polysubstance use disorder and AML suggests her immunocompromised state made her more susceptible to infection. Furthermore, tracheal-tube respiratory infections like pneumonia in hospitalized patients increase the risk of drug resistant M. abscessus. Long-term outcomes of quadruple therapy can stem from the individual effects of each drug or the development of multidrug resistance by bacterial microevolution. This case demonstrates the need for further research into the effect of immunosuppression from chemotherapy and substance use on susceptibility and response to treatment of M. abscessus infections.