Abstract
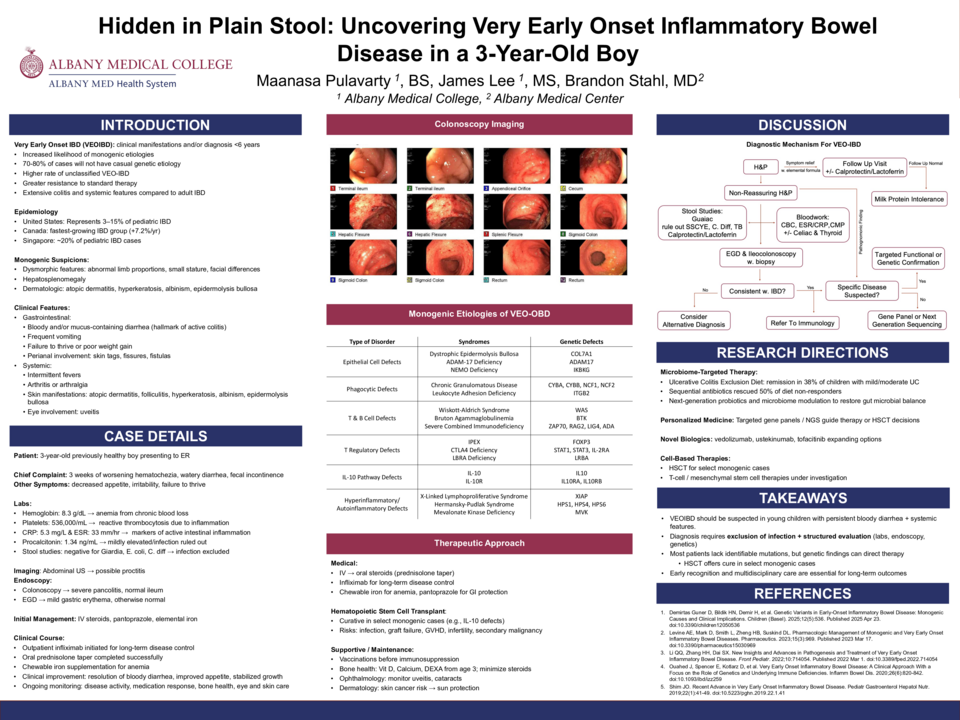
A previously healthy 3-year-old male presented to the ED with three weeks of progressively worsening hematochezia. He had been in his usual state of health until the mother noted bright red blood mixed in his stool. Over the following days, he developed increasingly frequent bloody bowel movements, up to ten daily, associated with loose stools and fecal incontinence. Review of systems was negative except for fecal incontinence, decreased appetite, and irritability. Initial workup by the PCP included testing for Giardia, E. coli, and fecal lactoferrin, all of which were negative. There were no recent dietary changes, travel, camping, or exposure to untreated water, and no personal or family history of inflammatory bowel disease or other gastrointestinal disorders. In the ED, labs showed a hemoglobin of 8.3 g/dL, platelets of 536,000/µL, CRP of 5.3 mg/L, ESR of 33 mm/hr, and procalcitonin of 1.34 ng/mL. Stool enteric pathogen panel and C. diff testing were negative. Abdominal ultrasound showed possible proctitis but was otherwise normal. Given the concern for colitis, gastroenterology was consulted for urgent endoscopic evaluation. The patient was admitted and started on IV methylprednisolone and pantoprazole. He was also started on elemental iron supplementation for anemia secondary to blood loss. Quantiferon Gold and hepatitis B serologies were sent in anticipation of biologic therapy. Colonoscopy revealed severe pancolitis with normal ileal mucosa. Concurrent EGD showed a grossly normal esophagus, stomach, and duodenum aside from minor areas of mild erythema. The patient continued on methylprednisolone and pantoprazole and showed clinical improvement. The patient was discharged home with outpatient GI follow-up, oral prednisone, and iron supplementation.
Very early onset inflammatory bowel disease (VEOIBD), defined as IBD diagnosed before six years of age, represents a rare but increasingly recognized subset of pediatric IBD. It often presents with extensive colitis, atypical extraintestinal manifestations, and a resistance to standard therapies. Advances in genetic testing have identified mutations in IL-10 signaling, epithelial barrier function, and T-cell regulation. Whole exome sequencing has directed personalized therapies through the identification of mutations in genes such as IL10RA/B, XIAP, and FOXP3. Studies are additionally investigating the role of intestinal microbial imbalance and innate immune dysfunction in VEOIBD manifestation. Potential areas for future research include further identifying genetic drivers, refining microbiome-targeted interventions, and understanding how early life-factors influence disease onset and progression. This case reinforces the importance of early detection and tailored treatment strategies in the management of VEOIBD.