Abstract
Background
Adverse Childhood Experiences (ACEs) are a set of ten prevalent exposures to abuse, neglect, and social challenges that can lead to toxic stress and an increased risk of chronic health conditions across the life course. According to recent studies, ACEs are remarkably common, with 61% of adults having at least one ACE and 1 in 6 adults reporting having experienced four or more ACEs. Even more alarmingly, at least five of the ten leading causes of death in the United States are associated with ACEs (CDC, 2021). Residents of Service Planning Area (SPA) 1 of Los Angeles County face unique health disparities due to limited community resources, geographic isolation, and difficulties in recruiting and retaining skilled health professionals. Data on the prevalence of ACEs in the Antelope Valley is limited and often extrapolated from larger county-wide data.
Study Design
The aim of this quality improvement study is to assess whether interventions documented by clinicians in response to ACE screenings lead to service utilization by pediatric patients. A retrospective chart review study design captures the comprehensive patient journey from initial time of screening to closed-loop referrals, identifying potential gaps that prevent service utilization. Patient documentation review of PEARLS reports spans March 2020 through May 2024. The study population is SPA-1 residents receiving care at High Desert and Olive View between the ages of 0-20, with 60% identifying as Hispanic/Latine. The three primary questions are: was a planned referral noted during screening, was the patient connected to services following screening, and what is the follow up status of the patient. Referrals are categorized into five subheadings: mental health, department of children and family services (DCFS), nutrition/sleep, and behavioral health. Follow up status was grouped into resolved, unresolved, in progress, or lost to follow up.
Results
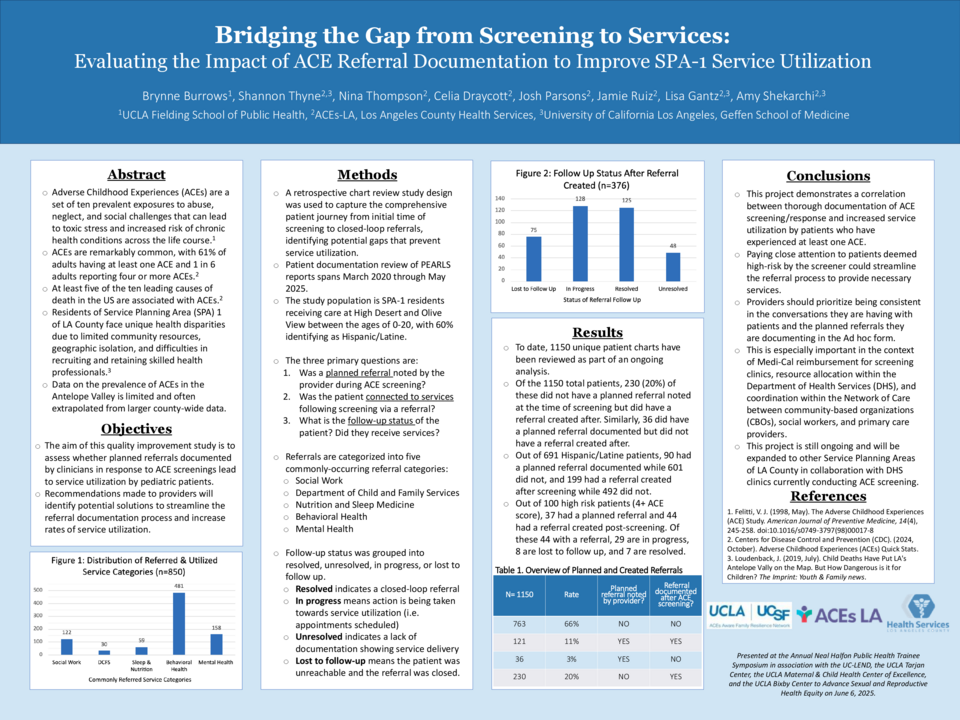
To date, 740 unique patient charts have been reviewed as part of an ongoing analysis. Preliminary data has found that 426 had a planned referral documented at or after initial ACE screening, with 181 having a referral created, 64 utilizing services, 76 in progress towards service utilization, 23 lost to follow up and 18 unresolved. Of the 446 (60%) total patients screened who identified as Hispanic/Latine, 51 (11%) had an ACE score of 4+ and 113 (25%) of them utilized services. Of the 95 high risk patients (ACE score of 4+), only 36 of them received a planned referral during screening and 41 were connected to services.
Discussion
Effective documentation by providers is critical in the ACEs screening and response process. Paying close attention to patients deemed high-risk by the screener could streamline the referral process to provide necessary services. This project demonstrates a correlation between thorough and timely documentation of ACE screening/response and increased service utilization by patients who have experienced at least one ACE. This is especially important in the context of Medi-Cal reimbursement for screening clinics, resource allocation within the Department of Health Services (DHS), and coordination within the Network of Care between community-based organizations (CBOs), social workers, and primary care providers.