Abstract
Background
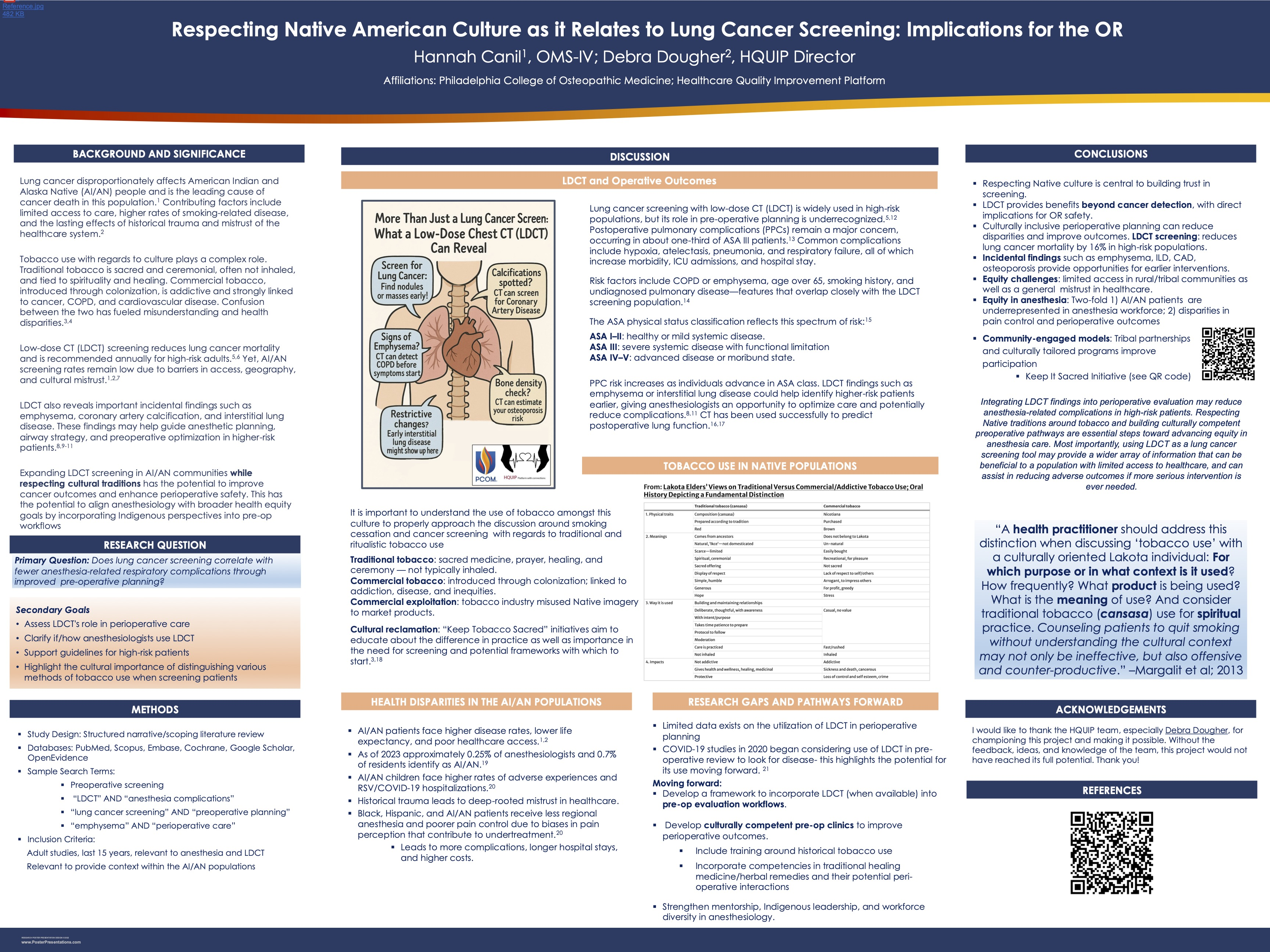
Lung cancer remains the leading cause of cancer death among American Indian and Alaska Native (AI/AN) people. They face higher rates of smoking-related disease, limited access to care, and a longstanding mistrust of the healthcare system. Confusion regarding tobacco use complicates both smoking cessation counseling and cancer screening conversations. Traditional tobacco holds cultural and spiritual significance and is not typically inhaled, while commercial tobacco is addictive and tied to cancer and cardiopulmonary disease. Low-dose CT (LDCT) screening has been shown to reduce lung cancer mortality by about 16% in high-risk groups. Utilization remains low in AI/AN communities. Importantly, LDCT often identifies incidental findings such as emphysema, coronary calcification, and interstitial lung disease, which may help guide anesthetic planning and reduce perioperative risk.
Objective
This project explores whether LDCT screening is used to reduce anesthetic respiratory complications through improved preoperative planning, while exploring the cultural considerations needed to advance equity in AI/AN populations.
Methods
A narrative review was conducted using PubMed, Scopus, Embase, Cochrane, Google Scholar, and OpenEvidence. Search terms included “LDCT and anesthesia complications,” “lung cancer screening and preoperative planning,” and “emphysema and perioperative care.” Adult studies published in the last 15 years were included, particularly in the context of AI/AN populations.
Results
Literature suggests that LDCT not only reduces lung cancer mortality in high-risk groups but also identifies incidental findings relevant for anesthesia. For example, emphysema and interstitial lung disease have been shown to predict postoperative pulmonary complications such as hypoxia, pneumonia, and respiratory failure. Additionally, findings such as coronary calcifications can help screen for cardiovascular disease. This allows anesthesiologists to anticipate challenges, adequately plan airway and ventilation strategies, and optimize patients before surgery. Despite these potential benefits, AI/AN populations continue to face significant barriers to screening, including geographically limited access to care and historical mistrust in the healthcare system. AI/AN patients also experience disparities in perioperative care, such as lower rates of regional anesthesia and poorer pain control, which contribute to worse outcomes. The literature highlights that culturally tailored initiatives, such as the Keep Tobacco Sacred campaign, are critical for improving screening participation by acknowledging the distinction between traditional and commercial tobacco use as well as sensitivity to traditional healing practices and their potential impact on operative success. Integrating LDCT into preoperative evaluation with cultural competence has the potential to reduce complications while building trust and advancing equity in anesthesia care.
Conclusion
Integrating LDCT findings into perioperative evaluation may reduce anesthetic complications in high-risk patients. Respecting Native traditions and building culturally competent preoperative pathways are essential steps toward advancing equity in anesthesia care. Most importantly, using LDCT as a lung cancer screening tool may provide a wider array of information that can be beneficial to a population with limited access to healthcare, and can assist in reducing adverse outcomes in future cases.