Abstract
Introduction
Thymomas are rare thymic tumors often associated with various autoimmune syndromes, most commonly myasthenia gravis. However, their association with hyperthyroidism and multinodular goiter has not been extensively reported. We present a rare case of a patient undergoing total thyroidectomy with median sternotomy for mediastinal goiter causing tracheal stenosis in the setting of hyperthyroidism secondary to toxic multinodular goiter, with an incidental intraoperative finding of thymoma, which was later diagnosed as a stage 1 type AB thymoma.
Case Presentation
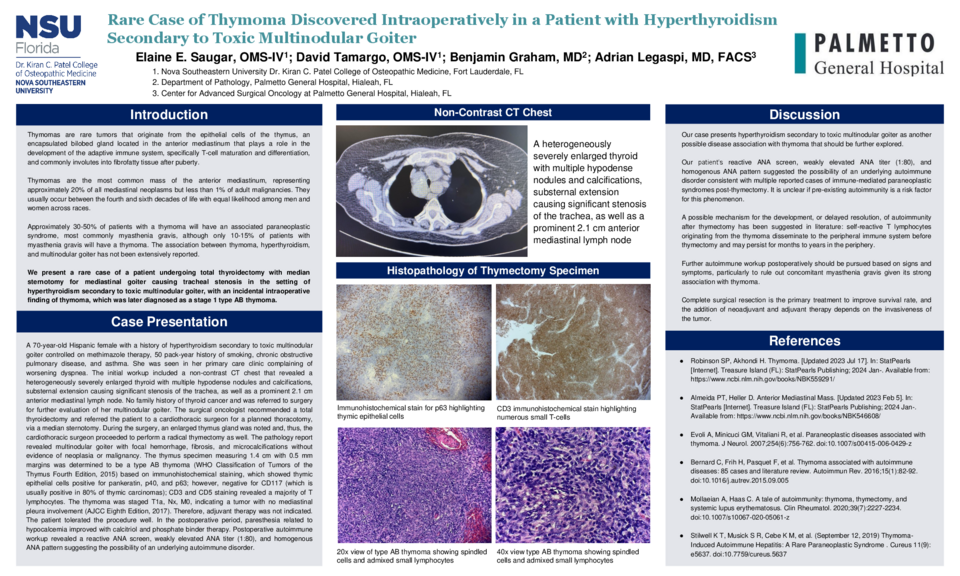
A 70-year-old Hispanic female with a history of hyperthyroidism secondary to toxic multinodular goiter controlled on methimazole therapy, 50 pack-year history of smoking, chronic obstructive pulmonary disease, and asthma. She was seen in her primary care clinic complaining of worsening dyspnea. The initial workup included a non-contrast CT chest that revealed a heterogeneously severely enlarged thyroid with multiple hypodense nodules and calcifications, substernal extension causing significant stenosis of the trachea, as well as a prominent 2.1 cm anterior mediastinal lymph node. No family history of thyroid cancer and was referred to surgery for further evaluation of her multinodular goiter. The surgical oncologist recommended a total thyroidectomy and referred the patient to a cardiothoracic surgeon for a planned thoracotomy, via a median sternotomy. During the surgery, an enlarged thymus gland was noted and, thus, the cardiothoracic surgeon proceeded to perform a radical thymectomy as well. The pathology report revealed multinodular goiter with focal hemorrhage, fibrosis, and microcalcifications without evidence of neoplasia or malignancy. The thymus specimen measuring 1.4 cm with 0.5 mm margins was determined to be a type AB thymoma (WHO Classification of Tumors of the Thymus Fourth Edition, 2015) based on immunohistochemical staining, which showed thymic epithelial cells positive for pankeratin, p40, and p63; however, negative for CD117 (which is usually positive in 80% of thymic carcinomas); CD3 and CD5 staining revealed a majority of T lymphocytes. The thymoma was staged T1a, Nx, M0, indicating a tumor with no mediastinal pleura involvement (AJCC Eighth Edition, 2017). Therefore, adjuvant therapy was not indicated. The patient tolerated the procedure well. In the postoperative period, paresthesia related to hypocalcemia improved with calcitriol and phosphate binder therapy. Postoperative autoimmune workup revealed a reactive ANA screen, weakly elevated ANA titer (1:80), and homogenous ANA pattern suggesting the possibility of an underlying autoimmune disorder.
Discussion
Our case presents hyperthyroidism secondary to toxic multinodular goiter as another possible disease association with thymoma. Additionally, postoperative autoimmune workup based on signs and symptoms, particularly to rule out concomitant myasthenia gravis given its strong association with thymoma, should be considered as immune-mediated paraneoplastic syndromes have been reported to develop post-thymectomy. It is unclear if pre-existing autoimmunity is a risk factor for this phenomenon.




