Abstract
Introduction: High-dose methylprednisolone has traditionally been used in brain-dead organ donors to improve hemodynamic status and reduce harmful inflammatory stress on organs. Based on the concern that such blasts of steroids may increase insulin requirements, coupled with the existing protocol of low-dose steroid treatment in other patient populations, Mid-America Transplant Services changed their donor management protocol from high-dose methylprednisolone to a lower dose of hydrocortisone. We sought to compare the hemodynamic stability, lung function, organ yield, and glycemic control of donors before and after this change to evaluate if a low-dose treatment regimen would be as effective in managing donors.
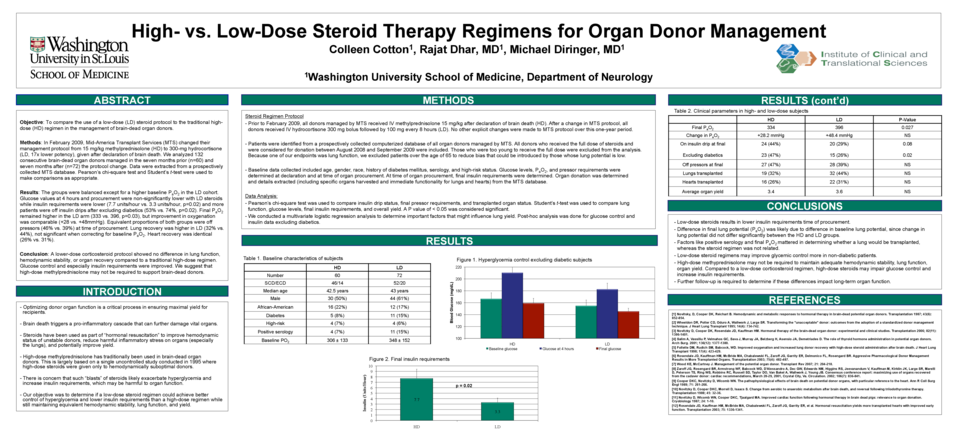
Methods: We analyzed 132 consecutive brain-dead organ donors between 8/2008 and 9/2009, including 60 patients treated prior to the protocol change (high-dose group) and 72 treated after (low-dose group). Change in PO2, change in glucose, final insulin requirements, final pressor requirements, and organ yield were extracted from a prospectively collected MTS database.
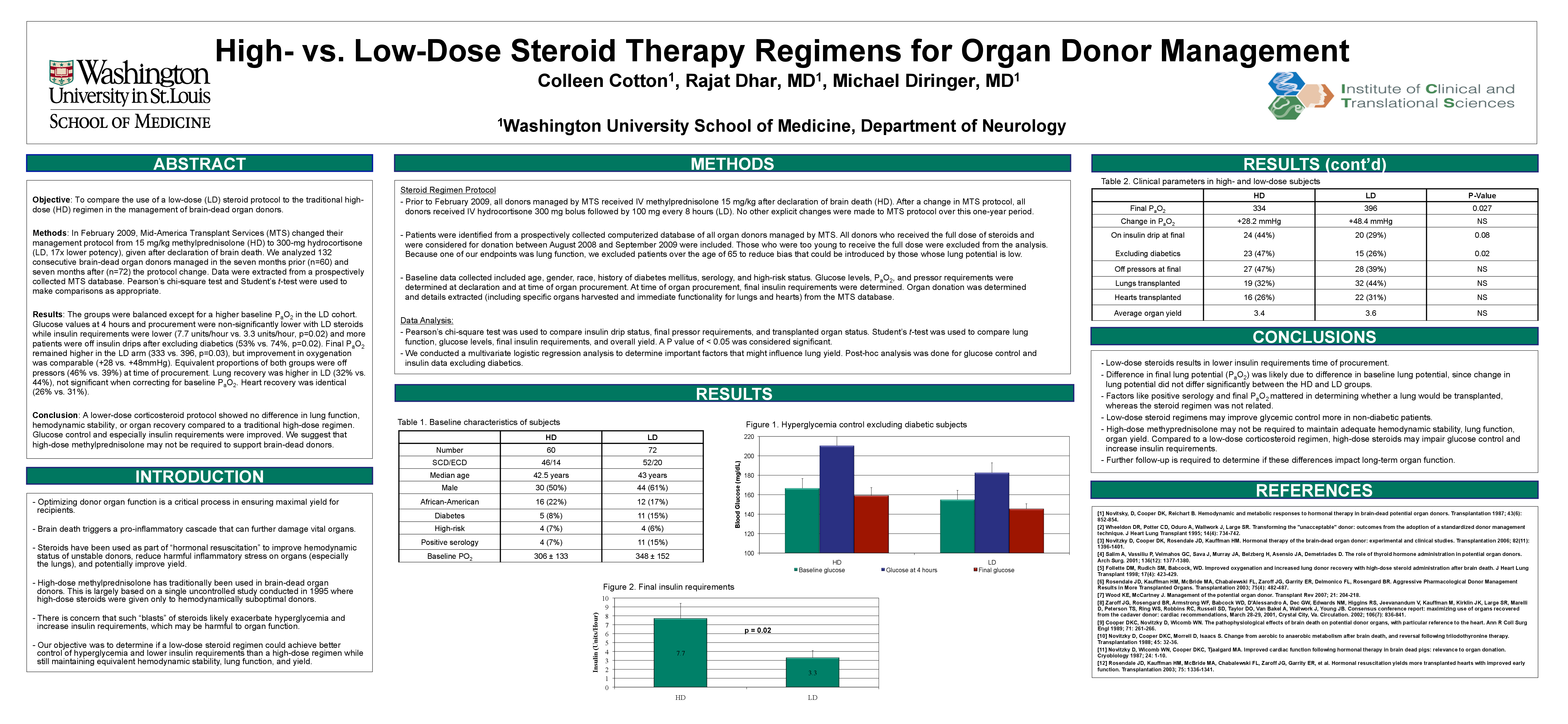
Results: Average final insulin requirements were greater in the high-dose group (7.7 units/hr vs. 3.3 units/hr, p = 0.02). Final pressor requirements, improvement in lung function, organ yield, and glucose control were not different.
Conclusions: The use of a low-dose steroid regimen for organ donor management was associated with and equivalent hemodynamic stability, equivalent lung function, equivalent organ yield, and improved glycemic control. This suggests that high-dose steroid treatment may not be required to support brain-dead organ donors. Further data on organ performance and confirmatory studies are required.