Abstract
Background:
Anxiety disorders are common in children with 7.8% of children and adolescents are diagnosis: leading to
academic impairment, substance misuse, unemployment in adulthood and other sequalae. In 2022, the United
States Preventive Services Task Force (USPSTF) recommended childhood anxiety screening (CAS) for children
8–18 years old. Early data at a large community health center (CHC) suggested that CAS was not routinely
performed, and a quality improvement (QI) project was initiated.
Aims:
The goals of the QI initiative were to increase knowledge and practice of CAS among family medicine
residents.
Methods:
The QI initiative is conducted at Community Health of South Florida, Inc. (CHI), a CHC serving over 61,000
patients from medically vulnerable populations.
The initiative is guided by the Plan-Do-Study-Act (PDSA) model which incorporates a four-step method for
implementing practice change.
In March through May 2023, the QI team developed and administered a needs assessment to ascertain
knowledge of pediatric screening recommendations, self-reported practices, and existing barriers. Though
residents were assessed on multiple recommendations, the QI team focused on CAS using the Screen for
Childhood Anxiety Related Emotional Disorders (SCARED), embedded in the electronic health record (EHR).
In October to November 2023, the QI team developed and delivered a training program to family medicine
residents on USPSTF recommendations, components and interpretation of the Screen for Childhood Related
Emotional Disorders (SCARED), and corresponding EHR navigation.
Outcomes were evaluated at three time-points. First, a pre- and post-training survey was administered. Second,
a baseline (August to November 2023) and post-intervention (November 2023 to January 2024) chart-review
was conducted. Third, a follow up knowledge-and-practice survey was administered. (January 2024).
Results:
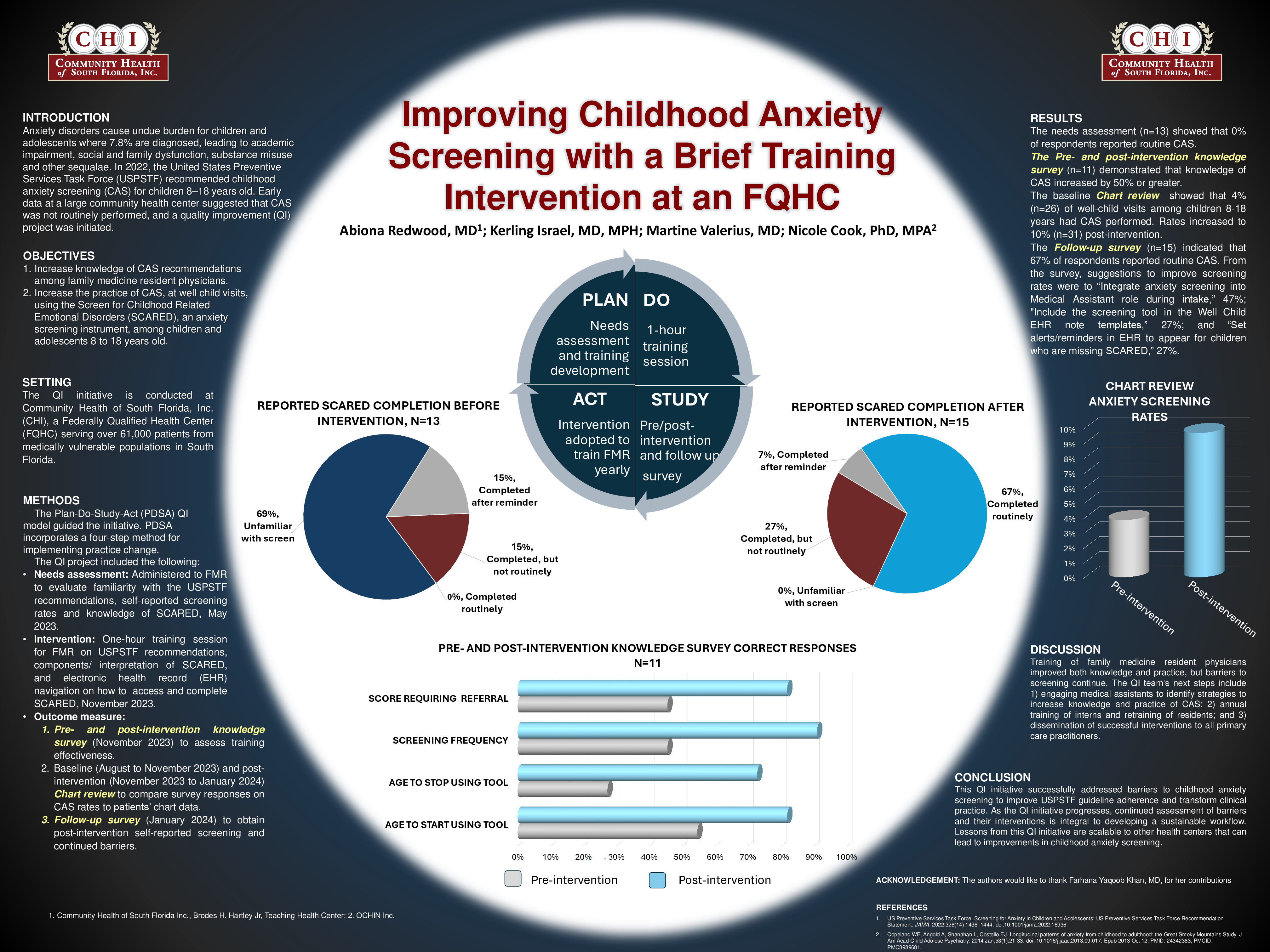
The needs assessment (n=13) indicated that 0% of respondents reported routine CAS, 36% did not know
screening recommendations and 36% were unaware of how to access SCARED in the EHR.
The pre- and post-training survey (n=11) demonstrated that knowledge of CAS increased 50% or greater.
The baseline chart review showed that 4% of well-child visits among children 8-18 had CAS performed. Rates
increased to 10% post-intervention.
The follow up knowledge-and-practice survey (n=15) indicated that 67% of respondents reported routine CAS,
27% did not know screening recommendations and 7% were unaware of how to access SCARED in the EHR.
Respondents (47%) recommended engaging medical assistants, to complete SCARED, for ongoing improvement.
Discussion:
Training of resident physicians improved both knowledge and practice, but barriers to screening continue. The
QI team’s next steps include 1) engaging medical assistants to identify strategies to increase knowledge and
practice of CAS; 2) annual training of interns and retraining of residents; and 3) dissemination of successful
interventions to all primary care practitioners.
Conclusion:
This QI initiative addressed anxiety screening barriers to improve USPSTF guideline adherence thus
transforming clinical practice. As the QI initiative progresses, continued assessment of barriers and their
interventions is integral to developing a sustainable workflow. Lessons from this QI initiative are scalable to
other health centers, thus leading to improvements in CAS.