Learning Curve Analysis and Favorable Perioperative Outcomes in Robot-Assisted versus Pure Laparoscopic Partial Nephrectomy
Abstract
Introduction and Objective: Robotic-assisted laparoscopic partial nephrectomy (RALPN) is emerging as a minimally invasive alternative of nephron sparing surgery but few data exist comparing it to pure laparoscopic partial nephrectomy (LPN). It was the objective of this analysis to evaluate perioperative outcomes of patients undergoing LPN and RALPN and investigate the learning curve (LC).
Methods: The Johns Hopkins Minimally Invasive Urological Surgery Database (1994-present) was queried for LPN. 150 patients were identified who underwent laparoscopic or robot-assisted laparoscopic partial nephrectomy (RALPN) for a single surgeon (MEA) since 2006. Preoperative patient and operative data were evaluated among LPN and RALPN using appropriate comparative tests. Learning curve for LPN and RALPN was investigated by examining operative times, warm ischemia time (WIT) and estimated blood loss (EBL) in groups of 25 consecutive patients. To account for combined learning curve, perioperative outcomes of patients operated on in 2009 or later were compared.
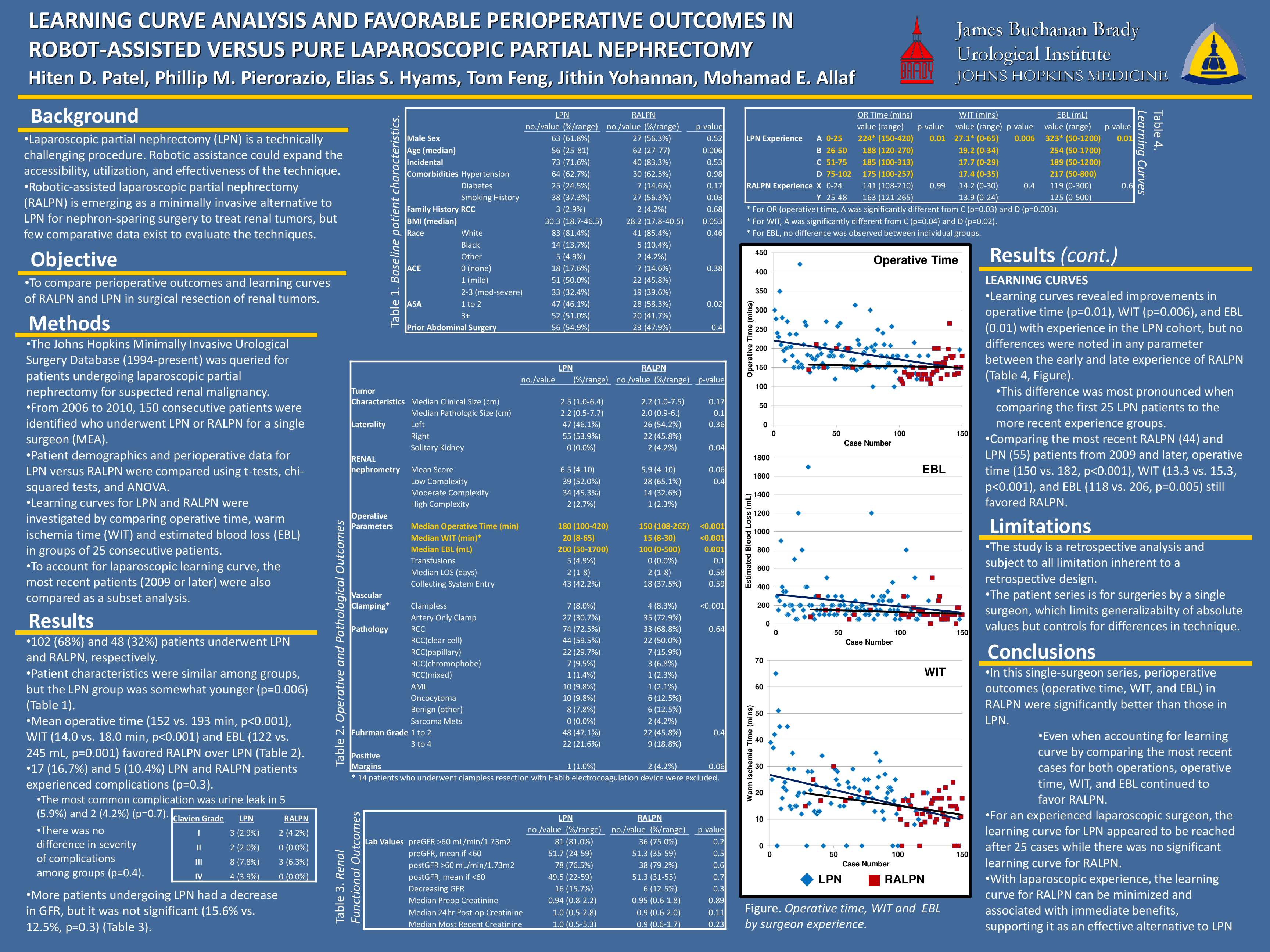
Results: 102 and 48 patients underwent LPN and RALPN respectively. Patient characteristics were similar among groups: 63 (61.8%) and 27 (56.3%) were men respectively, 33 (32.4%) and 19 (39.6%) had ACE scores of 2-3 (p=0.38), however 28 (58.3%) of RALPN and 47 (46.1%) of LPN had an ASA of 1-2 (p=0.02). Mean operative time (152 vs. 193 mins, p<0.001), WIT (14.0 vs. 18.0, p<0.001) and EBL (122 vs. 245, p=0.001) favored RALPN. A greater proportion of patients undergoing LPN had a decrease in GFR (15.6% vs. 12.5%, p=0.3). 17 (16.7%) and 5 (10.4%) complications occurred in LPN and RALPN respectively (p=0.3). Improvements in operative time (p=0.01), WIT (p=0.006) and EBL (0.01) were noted as experienced increased in the LPN. This difference was most pronounced when comparing the first 25 LPN patients to the more recent experience groups; there were no differences noted between the early and late experience of RALPN. 55 and 44 patients underwent LPN and RALPN respectively since 2009. Operative time (150 vs. 182, p<0.001), WIT (13.3 vs. 15.3, p<0.001) and EBL (118 vs. 206, p=0.005) favored RALPN in the most recent cohort.
Conclusions: RALPN has shorter operative and ischemia times, and less blood loss when compared to LPN. The LC for LPN appeared to be reached after 25 cases. Subsequently, transition from LPN to RALPN can be undertaken without an additional LC and be associated with immediate benefits.
Related articles