Abstract
Introduction:
Acute pancreatitis (AP) refers to inflammation of the pancreas and can be caused by gallstones, alcohol, ERCP, trauma, hypercalcemia, drugs, etc [1, 2]. However, AP secondary to Sildenafil has not been described previously.
Case Presentation:
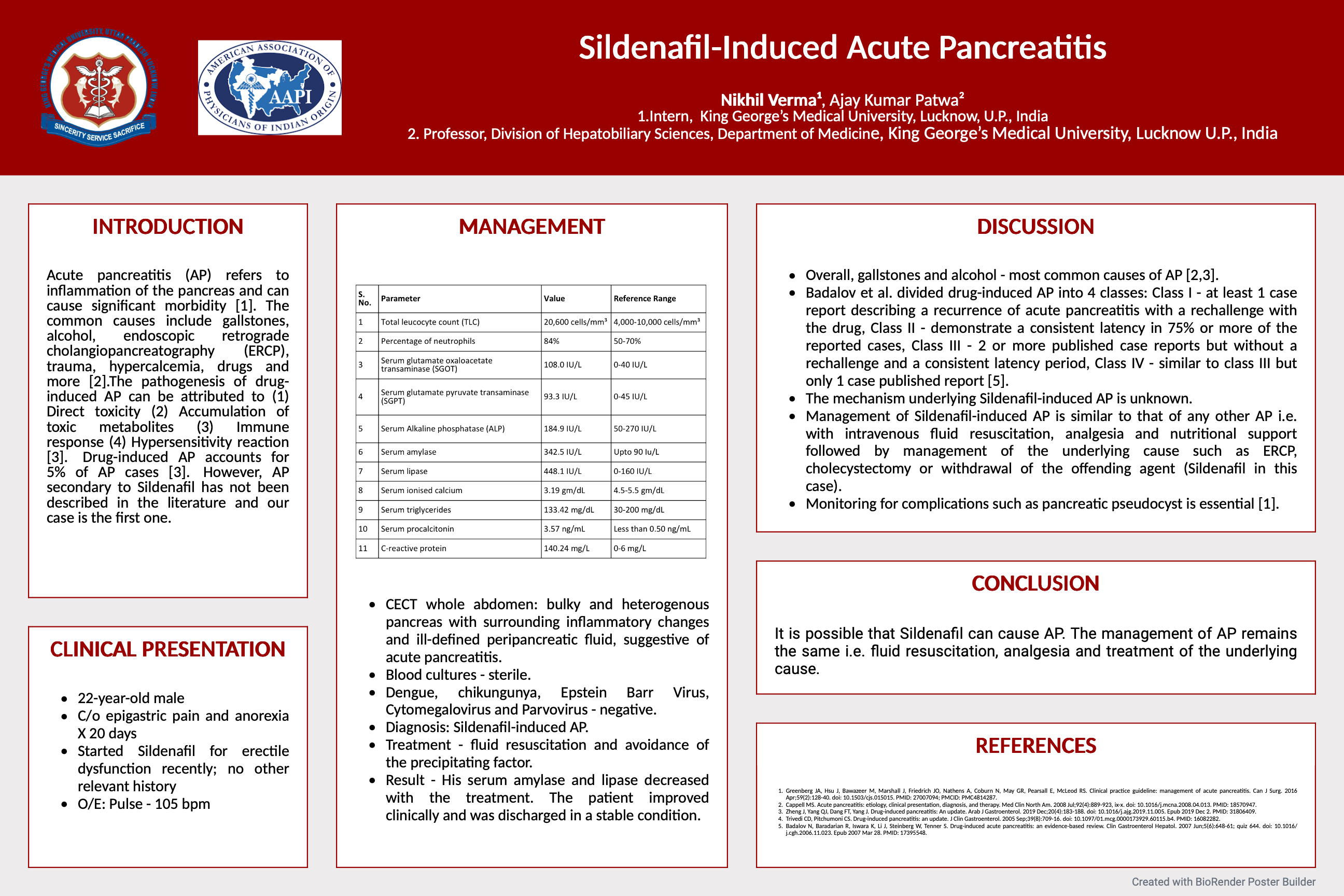
A 22-year-old male presented with epigastric pain and anorexia for 20 days. There was no history of insect bites, trauma, procedure, chronic illness, and alcoholism. He reported starting Sildenafil. TLC was 20,600 cells/mm3 with 84% neutrophils. SGOT, SGPT and ALP were 108.0 IU/L, 93.3 IU/L, and 184.9 IU/L respectively. Serum amylase was 342.5 IU/L and serum lipase was 448.1 IU/L. Serum ionised calcium, triglycerides, procalcitonin and CRP were 3.19 gm/dL, 133.42 mg/dL, 3.57 ng/mL and 140.24 mg/L respectively. CECT was suggestive of AP. Blood cultures were sterile. Given the history and CECT finding, he was diagnosed with Sildenafil-induced AP and was managed with fluid resuscitation and withdrawal of the precipitating factor. Serum amylase and lipase decreased with the treatment and he improved clinically.
Discussion:
Badalov et al. (2007) classified AP: Class I - ≥1 case report describing a recurrence of AP with a rechallenge with the drug, Class II - demonstrate a consistent latency in 75% or more of the reported cases, Class III - ≥2 published case reports but without a rechallenge and a consistent latency period, Class IV - similar to class III but only 1 case published report [3]. The pathogenesis of drug-induced AP includes (1) Direct toxicity (2) Accumulation of toxic metabolites (3) Immune response (4) Hypersensitivity reaction [4]. Management of Sildenafil-induced AP is similar to that of any other AP i.e. with intravenous fluid resuscitation, analgesia and nutritional support followed by management of the underlying cause such as ERCP, cholecystectomy or withdrawal of the offending agent. Monitoring for complications such as pancreatic pseudocyst is essential [1].
References:
- Greenberg JA, Hsu J, Bawazeer M et al. Clinical practice guideline: management of acute pancreatitis. Can J Surg. 2016;59(2):128-40.
- Cappell MS. Acute pancreatitis: etiology, clinical presentation, diagnosis, and therapy. Med Clin North Am. 2008;92(4):889-923, ix-x.
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007;5(6):648-61; quiz 644.
- Zheng J, Yang QJ, Dang FT, Yang J. Drug-induced pancreatitis: An update. Arab J Gastroenterol. 2019;20(4):183-188.