Abstract
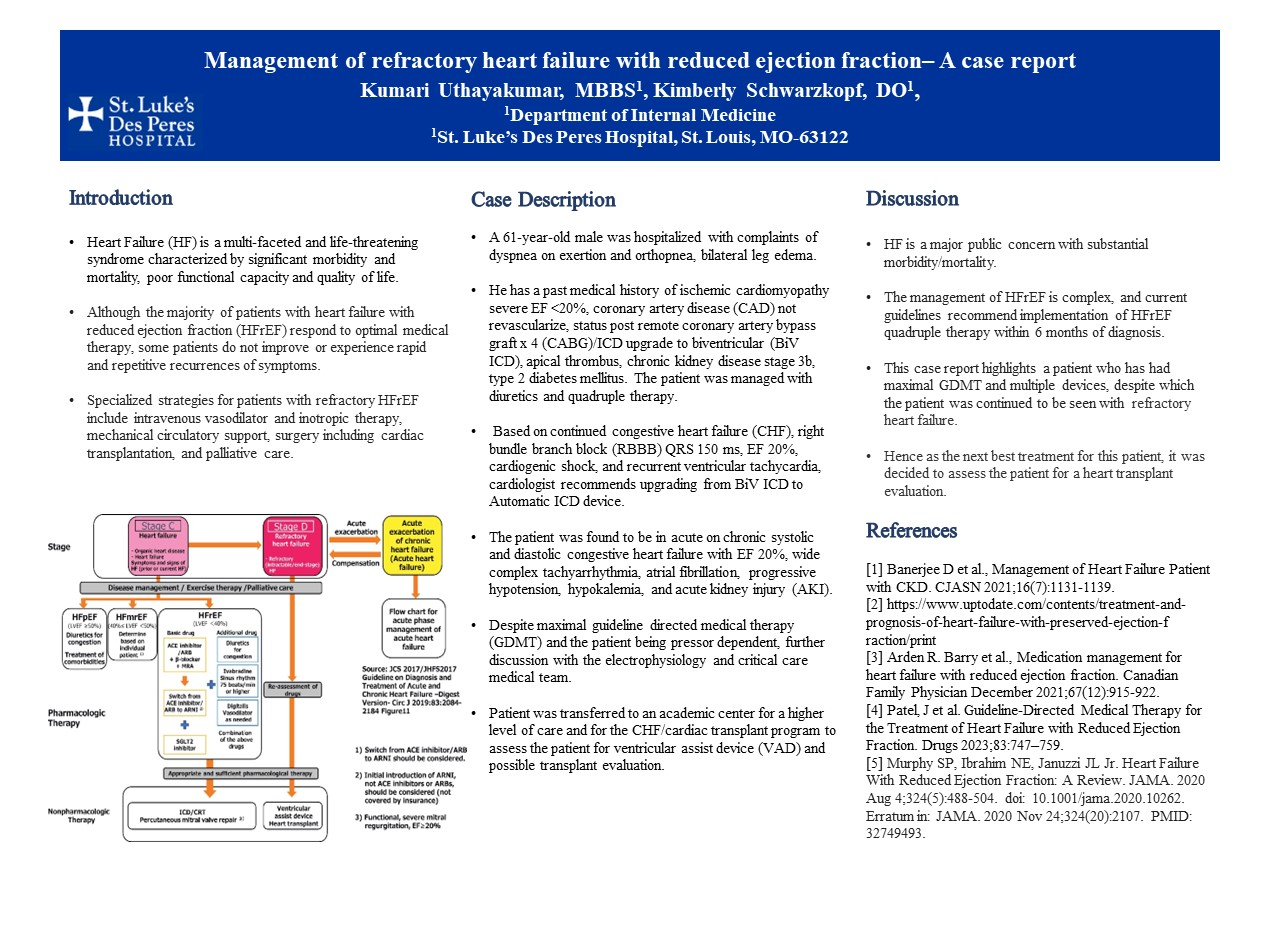
Introduction: Heart failure (HF) is a multi-faceted and life-threatening syndrome characterized by significant morbidity and mortality, poor functional capacity, and quality of life. Although the majority of patients with heart failure with reduced ejection fraction (HFrEF) respond to optimal medical therapy, some patients do not improve or experience rapid and repetitive recurrences of symptoms. Specialized strategies for patients with refractory HFrEF include intravenous vasodilator and inotropic therapy, mechanical circulatory support, surgery, including cardiac transplantation, and palliative care.
Case Description: A 61-year-old male was hospitalized with complaints of dyspnea on exertion, orthopnea, and bilateral leg edema He has a past medical history of ischemic cardiomyopathy, severe EF <20%, coronary artery disease (CAD) not revascularized, status post remote coronary artery bypass graft x 4 (CABG)/ICD upgrade to biventricular (BiV ICD), apical thrombus, chronic kidney disease stage 3b, type 2 diabetes mellitus. The patient was managed with diuretics and quadruple therapy. Based on continued congestive heart failure (CHF), right bundle branch block (RBBB) QRS 150 ms, EF 20%, cardiogenic shock, and recurrent ventricular tachycardia, the cardiologist recommends upgrading from BiV ICD to an automatic ICD device. The patient was found to be in acute chronic systolic and diastolic congestive heart failure with EF 20%, wide complex tachyarrhythmia, atrial fibrillation, progressive hypotension, hypokalemia, and acute kidney injury (AKI). Despite maximal guideline-directed medical therapy (GDMT) and the patient being pressure-dependent, further discussion with the electrophysiology and critical care medical teams is needed. The patient was transferred to an academic center for a higher level of care and for the CHF/cardiac transplant program to assess the patient for a ventricular assist device (VAD) and possible transplant evaluation.
Discussion: HF is a major public concern with substantial morbidity/mortality. The management of HFrEF is complex, and current guidelines recommend implementation of HFrEF quadruple therapy within 6 months of diagnosis. This case report highlights a patient who has had maximal GDMT and multiple devices, despite which the patient continued to be seen with refractory heart failure. Hence, as the next best treatment for this patient, it was decided to assess the patient for a heart transplant evaluation.