Abstract
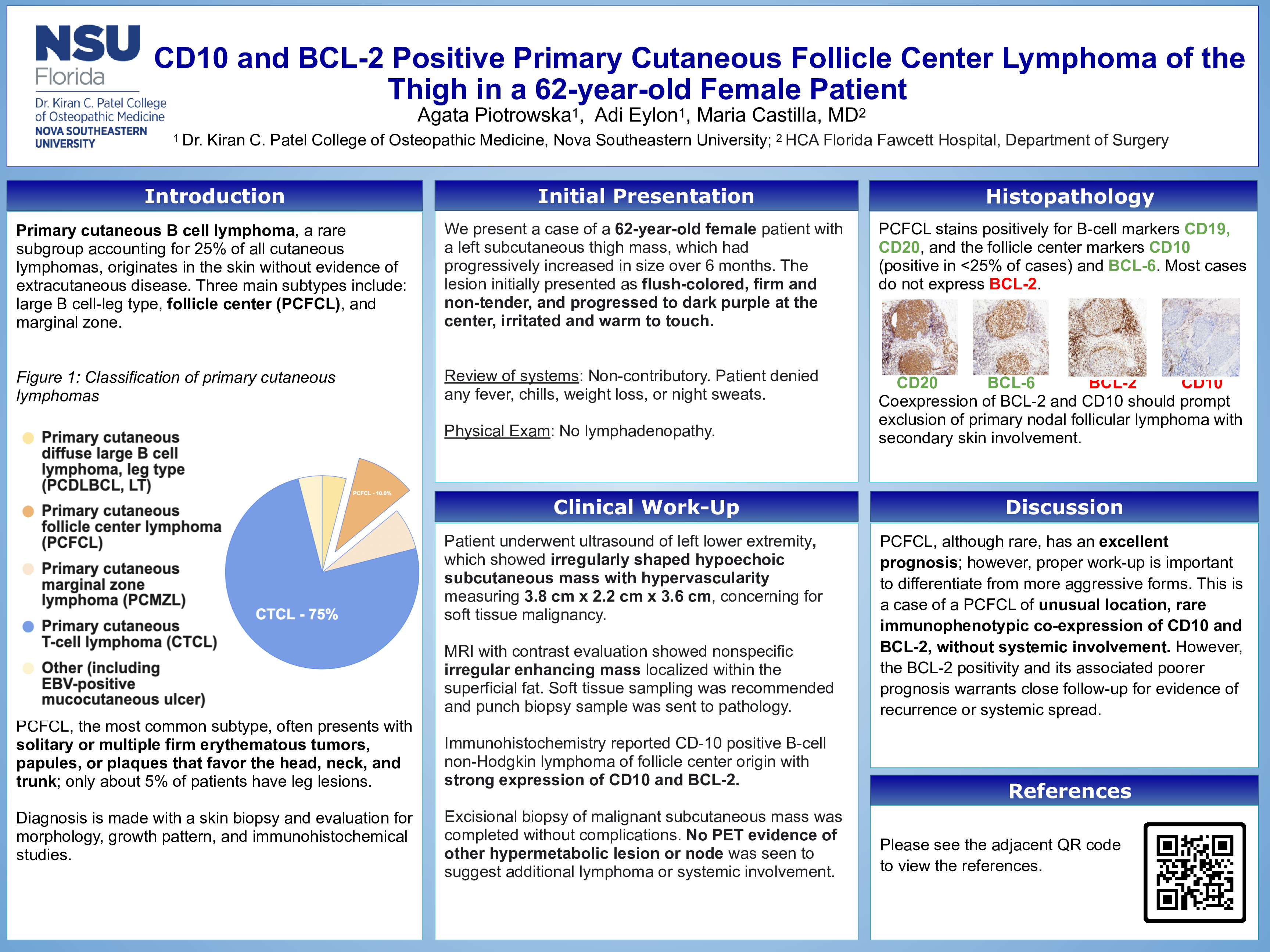
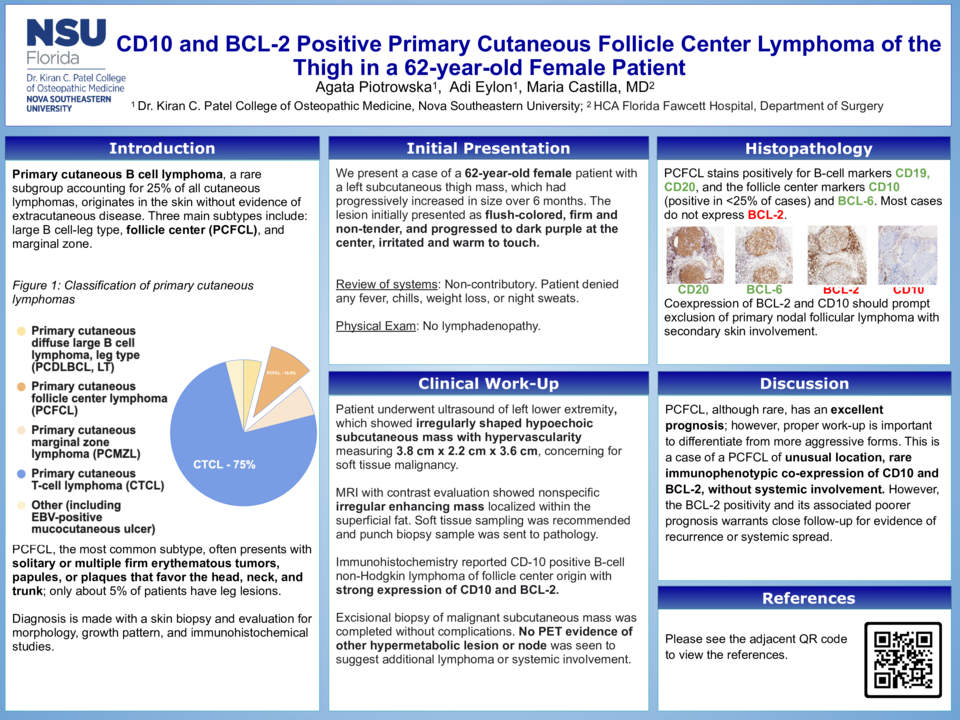
Introduction: Primary cutaneous B cell lymphoma, a rare subgroup accounting for 25% of all cutaneous lymphomas, originates in the skin without evidence of extracutaneous disease. Three main subtypes include: large B cell-leg type, follicle center (PCFCL), and marginal zone. PCFCL, the most common subtype, often presents with solitary or multiple firm erythematous tumors, papules, or plaques that favor the head, neck, and trunk; about 5% of patients have leg lesions. Diagnosis is made with a skin biopsy and evaluation for morphology, growth pattern, and immunohistochemical studies. PCFCL stains positively for B-cell markers CD19, CD20, and typically, the follicle center markers CD10 and BCL-6. Most cases do not express BCL-2, and coexpression of BCL-2 and CD10 should prompt exclusion of primary nodal follicular lymphoma with secondary skin involvement.
Case Description: We present a case of a 62-year-old woman who presented with a left subcutaneous thigh mass, which had progressively increased in size over 6 months. The lesion initially presented as flush-colored, firm and non-tender, and progressed to dark purple at the center, irritated and warm to touch. The patient denied systemic symptoms, like fever, weight loss, or night sweats. The lesion was evaluated with ultrasound, MRI, biopsy, neogenomics and FISH studies, which confirmed a diagnosis of B-cell non-Hodgkin lymphoma of follicular origin measuring 3.8 cm x 2.2 cm x 3.6 cm, expressing both CD10 and BCL-2. The patient subsequently underwent systemic workup, which was not suggestive of systemic disease.
Discussion: PCFCL, although rare, has an excellent prognosis; however, proper work up is important to differentiate from more aggressive forms. This is a case of a PCFCL of unusual location, rare immunophenotypic co-expression of CD10 and BCL-2, without systemic involvement. However, the BCL-2 positivity and its associated poorer prognosis warrants close follow-up for evidence of recurrence or systemic spread