Spinal Chordoma: First experiences of combined surgical and radiosurgical treatment with refined intra- and perioperative imaging
Abstract
Objective: Spinal chordomas are mostly sacrally located, invasive neoplasms arising from ectopic rests of notochordal tissue; sacrectomy with consecutive severe deficits is widely advocated the primary treatment. We analyzed a pilot series of patients with combined treatment by microsurgery and spinal robotic radiosurgery. Benefit of pre- and postoperative PET-CT-imaging, intraoperative CT-imaging (iCT) in combination with neuronavigation and clinical outcome were evaluated.
Methods: Five patients (4 sacral, one cervical chordoma; disease up to now: 52 38 mo) were operated alltogether ten times since 1/2007. None of the patients had severe neurological deficit at start of treatment in our clinic. Surgery was performed with iCT-imaging for resection control and exclusion of lesions of adjacent structures, and, in two patients, for generation of image data for navigation. Two patients have received conventional radiotherapy (60-68 Gy). In 4 patients remnant tumor masses with high operative risk were treated alltogether 13 times by spinal robotic radiosurgery (CyberKnife, Accuray; Ca, USA) In 3 patients repetitive PET/CT scans using [F-18]Fluordeoxyglucose (FDG) were performed.
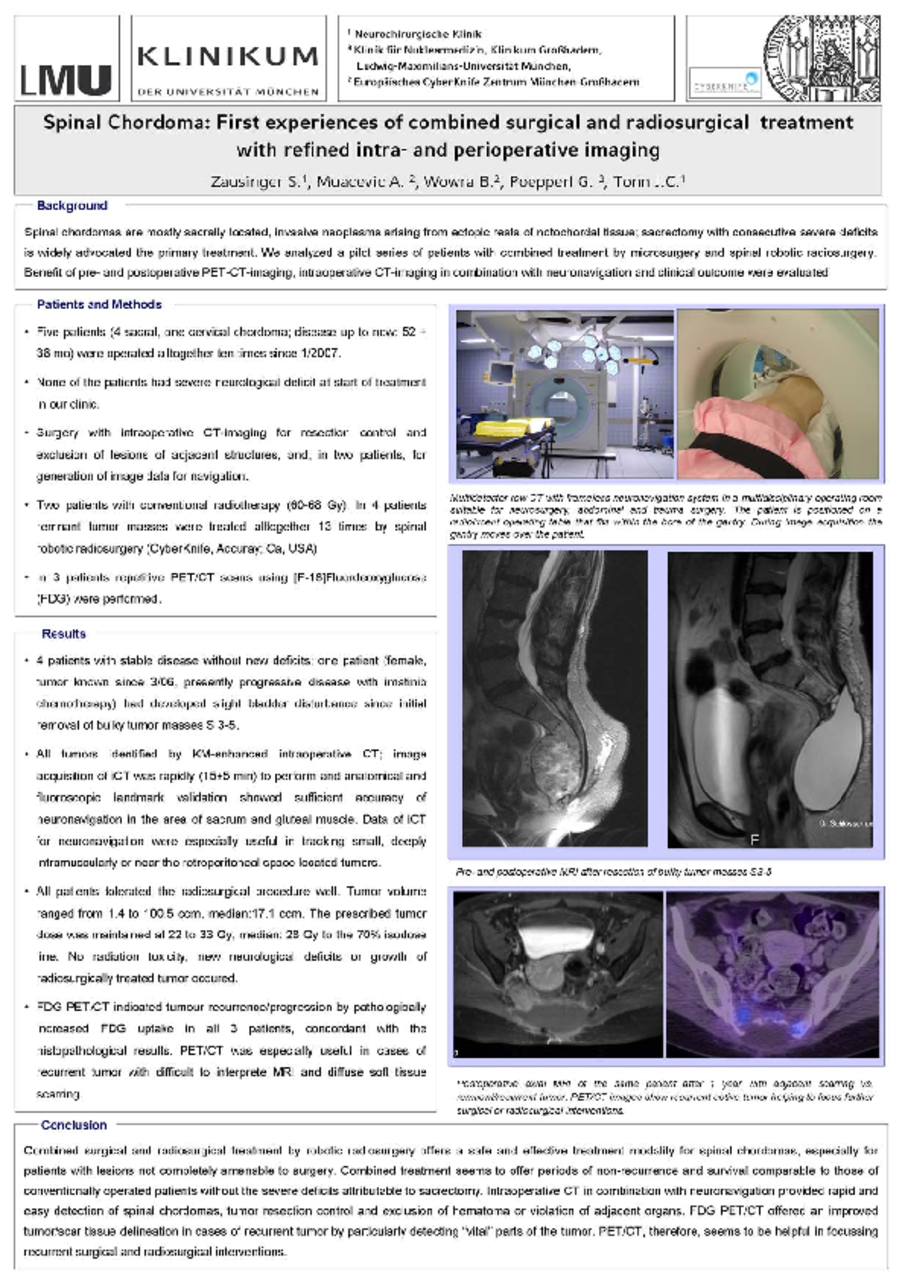
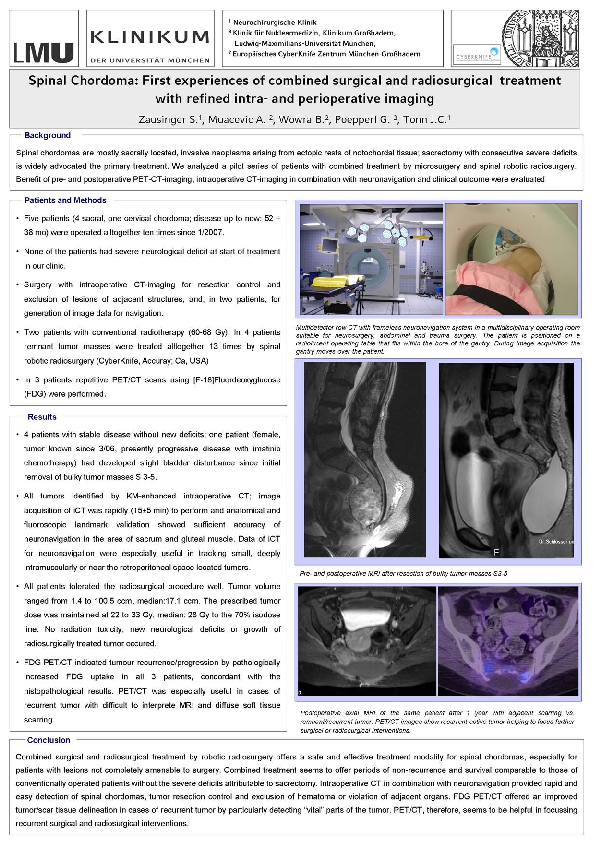
Results: In 4 patients there is stable disease up to now without new deficits; one patient (female, tumor known since 3/06, presently progressive disease with imatinib chemotherapy) had developed slight bladder disturbance since initial removal of bulky tumor masses S 3-5. All tumors could be identified by KM-enhanced iCT; image acquisition of iCT was rapidly (15±5 min) to perform and anatomical and fluoroscopic landmark validation showed sufficient accuracyy of neuronavigation of tumors, located in the area of sacrum, gluteal muscle and near the retroperitoneal space. All patients tolerated the radiosurgical procedure well. Tumor volume ranged from 1.4 to 100.5 ccm, median:17.1 ccm. The prescribed tumor dose maintained at 22 to 33 Gy, median: 28 Gy to the 70% isodose line. No radiation toxicity, new neurological deficits or growth of radiosurgically treated tumor occured. FDG PET/CT indicated tumour recurrence/progression by pathologically increased FDG uptake in all 3 patients, concordant with the histopathological results. PET/CT was especially useful in cases of recurrent tumor with difficult to interprete MRI and diffuse soft tissue scarring.
Conclusion: Combined surgical and radiosurgical treatment by robotic radiosurgery offers a safe and effective treatment modality for spinal chordomas, especially for patients with lesions not completely amenable to surgery. Combined treatment seems to offer periods of non-recurrence and survival comparable to those of conventionally operated patients without the severe deficits attributable to sacrectomy. Intraoperative CT in combination with neuronavigation provided rapid and easy detection of spinal chordomas, tumor resection control and exclusion of hematoma or violation of adjacent organs. FDG PET/CT offered an improved tumor/scare tissue delineation in cases of recurrent tumor by particularly detecting “vital” parts of the tumor. Helping to focus recurrent surgical and radiosurgical interventions.
Related articles