Abstract
Background: In 2019, stroke was the 5th most common cause of death in the United States. In the same year, Florida ranked 14th in the US in age-adjusted death from stroke rate per 100,000. Florida’s unique landscape gives rise to an opportunity to study stroke and its relationship to certain social determinants of health (SDoH). While other studies have analyzed factors like stroke mortality and urban vs. rural county classifications, there has been little done to correlate stroke rates in Florida with other SDoH.
Objective: This study examines the relationship between various county SDoH and the history of stroke across all 67 Florida counties. Variables studied include median income, family practitioners per capita, percentage of individuals with health insurance, individuals with a personal doctor, households within a half mile from recreational trails, households within a half mile from a healthy food source, smoking rates, and obesity rates.
Methods: We conducted a cross-sectional database study of all 67 counties in Florida utilizing county-specific data aggregated by FLHealthCHARTS. Data for “stroke history” was identified using the parameter “Adults who have ever been told they had a stroke” from the Florida Behavioral Risk Factor Surveillance System (BRFSS). Data on the eight health categories analyzed in this study was taken from the U.S. Census Bureau, Healthy People 2030, and the BRFSS. All data used in this study was from 2019, representing the latest year that data was available for all our criteria. Data was retrieved from these sources and analyzed in Microsoft Excel using an individual bivariate linear regression analysis that looked at a p-value <0.01, F statistic, and adjusted R squared value. An analysis comparing each SDoH to stroke history was performed independently by two researchers and cross-referenced for accuracy.
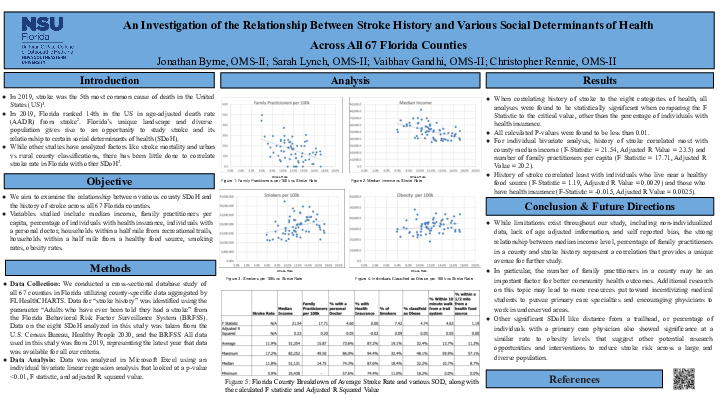
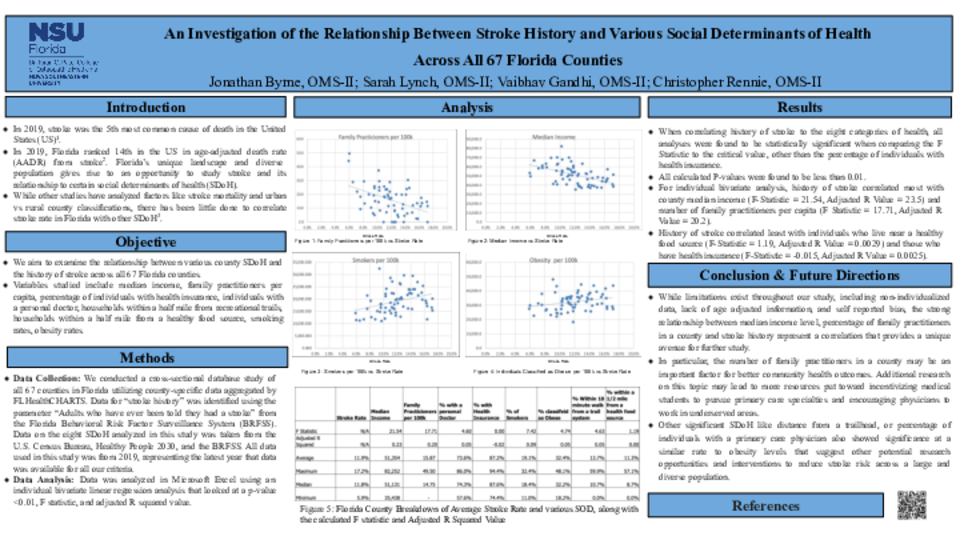
Results: When correlating history of stroke to the eight categories of health, all analyses were found to be statistically significant when comparing the F Statistic to the critical value. For each 17 individual bivariate analyses, history of stroke correlated most with county median income (F-Statistic = 21.54, Adjusted R Value = 23.5) and number of family practitioners per capita (F Statistic = 17.71, Adjusted R Value = 20.2) and least with individuals who live near a healthy food source (F-Statistic = 1.19, Adjusted R Value = 0.0029) and those who have health insurance (F-Statistic = -0.015, Adjusted R Value = 0.0025).
Conclusion: While limitations exist throughout our study including non-individualized data, lack of age adjusted information, and self-reported bias, the strong relationship between median income level, percentage of family practitioners in a county and stroke history represent a correlation that provides a unique avenue for further study. In particular, the number of family practitioners in a county may be an important factor for better community health outcomes. Additional research on this topic may lead to more resources put toward incentivizing medical students to pursue primary care specialties and encouraging physicians to work in underserved areas. Other significant SDoH like distance from a trailhead, or percentage of individuals with a primary care physician also showed significance at a similar rate to obesity levels that suggest other potential research opportunities and interventions to reduce stroke risk across a large and diverse population.