Abstract
Background: Minorities, particularly those of color, are faced with implicit biases by healthcare professionals that may impact their standard of care and quality of life. The study of dermatology has long been based on those of Caucasian skin color, unintentionally affecting the treatment of patients of color. Melanoma, although mostly curable, can become fatal in those presenting with advanced stages at diagnosis. Despite being rare in racial minorities, melanoma is associated with a worse prognosis than in White populations.
Objective: The objective of this study was to determine the role of education in preventing bias and improving detection and treatment of melanoma in minority groups to improve patient outcomes.
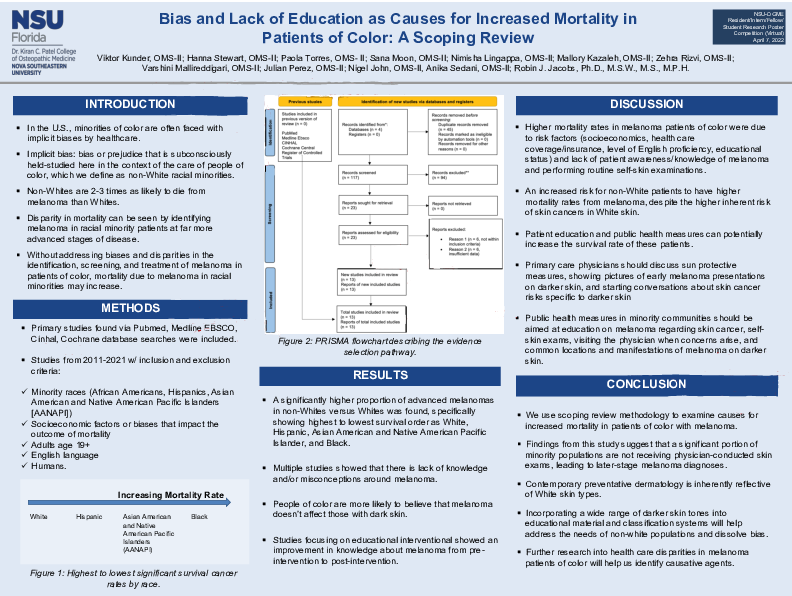
Methods: This study was designed as a scoping review to gather evidence on implicit bias and lack of education in the treatment of melanoma in people of color. Following PRISMA guidelines, we searched peer-reviewed literature involving melanoma, education, and treatment bias in people of color using databases PubMed & MEDLINE. We restricted the search to articles published in English and focused on patients of color who were treated for melanoma by a physician and limited all articles published before 2010. We used Boolean operators for our search, which combined terms as follows: “melanoma” AND “people of color” AND “education” OR “bias.” Our initial search yielded 117 articles after removing duplicates. After filtering based on inclusion and exclusion criteria, 25 articles were selected. Further analysis for relevance yielded 12 articles.
Results: The main domains for data extraction were 1) risk factors, 2) surveys of current knowledge, and 3) educational interventions. Multiple studies explored the risk factors associated with increased risk of mortality in melanoma and reported that non-Hispanic blacks were at increased risk of mortality and reported Medicare coverage as a risk factor for late-stage diagnosis when compared to commercial insurance and that compared to minorities, whites had more total body skin examinations. Four studies conducted educational-based surveys to assess current knowledge on melanoma and reported a lack of understanding and misconceptions on melanoma prevention and detection among minority groups of color; three of these used educational intervention to bridge these gaps in knowledge. These studies reported an improvement in understanding of melanoma risk factors, prevention, warning sign, and self-skin exams in minority populations.
Conclusion: This review identified socioeconomic factors, bias, and lack of education in minority populations as causes for increased mortality rates in melanoma. Moreover, preventative dermatology is largely based on Caucasian skin types, therefore, incorporating darker skin tones into education will dispel any implicit bias that may exist. Further, evidence determined that inherent patient knowledge and understanding of skin cancer is inaccurate and can be significantly improved through educational interventions, such as brochures and videos. Additional educational interventions may be beneficial to increase understanding of melanoma in populations of color to address health disparities in dermatological care.